Download
1 / 84
850 likes | 1.08k Views
Clinical Pathological Conference: Barrett ’ s Esophagus and Esophageal Carcinoma. Ralph Lee, MD, FRCPC (Division of Gastroenterology) Celia Marginean , MD (Department of Pathology) September 9 , 2014. Objectives (1). At the end of this lecture, the student will be able to:

E N D
Clinical Pathological Conference: Barrett’s Esophagusand Esophageal Carcinoma Ralph Lee, MD, FRCPC (Division of Gastroenterology) Celia Marginean, MD (Department of Pathology) September 9, 2014
Objectives (1) At the end of this lecture, the student will be able to: • Define Barrett’s esophagus. • Illustrate the underlying pathogenesis and clinical relevance of Barrett’s esophagus. • Discuss the epidemiology and risk factors for Barrett’s esophagus. • Identify the morphological features of GERD and Barrett’s esophagus. • Identify the morphological features of Barrett’s dysplasia (low grade, high grade). • Summarize the diagnosis and management of Barrett’s esophagus.
Objectives (2) • Classify the different types of esophageal tumours • Differentiate between the two primary types of esophageal carcinoma in terms of their epidemiology, etiology, clinical presentation, complications and prognosis. • Identify the morphological features of esophageal carcinoma (squamous and adenocarcinoma) • Outline the diagnosis, staging, management and prevention of the two primary types of esophageal carcinoma. • Describe the epidemiology, clinical presentation/diagnosis and management of eosinophilic esophagitis. • Identify the morphological features of eosinophilic esophagitis.
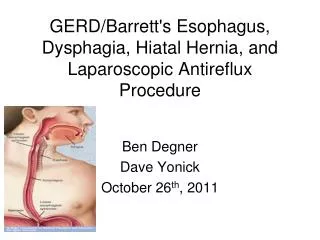
To Review… • GERD is a condition which develops when the reflux of stomach contents into the esophagus causes troublesome (i.e. adversely affecting a patient’s well-being) symptoms and/or complications. • Classic symptoms include heartburn and regurgitation • Presence of ‘Alarm features’ • Indicate when patients presenting with GERD-like symptoms should be further investigated vs. empiric treatment • ‘Alarm features’ for GERD • persistent vomiting, signs or symptoms of gastrointestinal blood loss, anemia, unintentional weight loss, dysphagia and a palpable epigastric mass.
Case 1 (1) • 50y.o. Caucasian male • RFR: Endoscopy for GERD • HPI: Longstanding (>15 years) history of heartburn, 3-4x/week, controlled with ranitidine (H2RA) prn. Denies dysphagia, odynophagia, nausea, vomiting, early satiety or weight loss. • PMx: Hypertension, hypercholesterolemia. No previous surgeries or endoscopies.
Case 1 (2) • Meds: Ranitidine 150mg poprn, Lipitor 10mg po OD, ASA 81mg po OD. All: NKDA • Habits: Smoking: 30 pack-years; Alcohol: 4 glasses wine/day • Family Hx: Non-contributory • Physical Exam: Obese, but otherwise normal. • Labs: CBC, electrolytes, BUN, Cr, LFTs, Iron studies N.
Case 1 (3) • Does this patient need an upper endoscopy? Why or why not? • YES! • Why (i.e. what indication)? • > 15 year history of GERD • Why does this matter? • 13 – 20% of patients undergoing endoscopy for chronic GERD will have Barrett’s esophagus • Why does Barrett’s esophagus matter?
Because this… …can turn into this. Barrett’s Esophagus Esophageal Adenocarcinoma
Barrett’s Esophagus (BE)Definition (1) • Definition • change in the distal esophageal epithelium of any length that: • Can be recognized as columnar type mucosa during endoscopy • Is confirmed to have intestinal metaplasia by biopsy of the tubular esophagus
Barrett’s Esophagus (BE)Definition (2) • Esophagus normally lined by stratified squamous epithelium which transitions to columnar mucosa at the squamocolumnar junction (SCJ; AKA Z-line)
Barrett’s Esophagus (BE)Definition (3) • In Barrett’s, columnar-appearing epithelium with intestinal metaplasia replaces the squamous epithelium
Why is this important?Clinical relevance • Barrett’s esophagus is a premalignant lesion for adenocarcinoma • 0.5%/year develop esophageal adenocarcinoma • (+) low-grade dysplasia 10 – 28% over 5 years • 1.8%/year (controversial) • (+) high-grade dysplasia 16 – 59% over 5 years • 6%/year • Higher risk of adenocarcinoma if > 2 cm of Barrett mucosa • Barrett’s esophagus is associated with quality of life
Barrett’s Esophagus (BE)Epidemiology and Risk Factors • Prevalence 23 – 376/100,000 • Another estimate: 1.6% of the population • Symptomatic (i.e. GERD): 2 – 18% • Risk Factors: • Age ≥ 50 • Male (2:1) • White race • Uncommon in blacks, Asians • Chronic GERD(> 10 years) • Hiatus hernia • Elevated BMI • Intra-abdominal distribution of body fat
Barrett’s Esophagus (BE)Clinical Presentation • GERD • Heartburn, regurgitation • Chest pain, cough, sore throat, water brash • Esophagitis, esophageal ulcers, strictures • Asymptomatic* • 44% of with patients with BE have not had troublesome heartburn and/or acid regurgitation in the past 3 months
Barrett’s Esophagus (BE)Diagnosis • Not a clinical diagnosis • Upper endoscopy (EGD) must be performed. • Two criteria must be met to diagnose BE: • Endoscopic evidence of columnar-appearing epithelium lining the distal esophagus above the GEJ • Histological biopsies from this area must show specialized intestinal metaplasia (goblet cells) • 4 quadrant biopsies every 1-2cm
What is an EGD?(Esophagastroduodenoscopy) • Patient administered topical anesthetic and/or conscious sedation • Flexible, fiber optic camera inserted into the oral cavity and guided down into the esophagus, stomach and duodenum • Instrument maneuvered by torqueing tube or using directional dials • Other features: • Air insufflation • Lens flush • Suction • Working channel • biopsies, snares, injections, cautery • Digital pictures, zoom, narrow band imaging
Barrett’s Esophagus (BE) Endoscopy (1) Normal Barrett’s Barrett’s
Barrett’s Esophagus (BE) Pathology
ESOPHAGUS Squamous epithelium Submucosa with mucus secreting glands Muscularispropria (inner circular and outer longitudinal layers ) GEJ
Gastroesophageal junction Squamous epithelium Gastric cardia columnar epithelium
ESOPHAGITIS • Epithelial damage due to inflammation • Most common cause is gastroesophagealreflux -GERD- (reflux of gastric contents into lower esophagus) • Infectious causes are much less common - Candida, herpes virus, CMV, bacteria (immunocompromised) • Chemical (erosive) esophagitis - acids, alkali • Eosinophilicesophagitis
GERD - Reflux esophagitis hyperemia • Most common; due to reflux of gastric contents into lower esophagus • Physiology: chronic exposure to gastric juices (acid) impairs reparative capacity of esophageal mucosa • Gross: severe cases exhibit hyperemic mucosa with focal hemorrhage
GERDelongated vascular papillae normal basal cell hyperplasia intraepithelial eosinophils
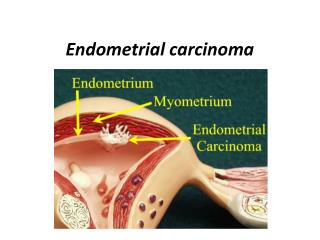
Barrett’s esophagus • Distal squamous mucosa is replaced by columnar epithelium with goblet cells (small intestinal type) as a response to prolonged injury = intestinal metaplasia • Columnar epithelium may be more resistant to acid, pepsin and bile Metaplasia = replacement of one type of normal epithelium by another type of normal epithelium usually not found at that location
Barrett’s esophagus Columnar epithelium with glands Goblet cells
BE Dysplasia • Dysplasia in BE is defined as unequivocal neoplastic epithelium confined to the basement membrane (intraepithelial neoplasia) • Invasion of basement membrane = invasive adenocarcinoma • Risk factors for dysplasia include increasing length of BE and increasing patient age • Pathologically, BE dysplasia is classified as: • negative • indefinite • positive for low dysplasia • positive for high-grade dysplasia • adenocarcinoma
Invasive adenocarcinoma Malignant glands invading the muscularis mucosae
Barrett’s Esophagus (BE) Management • Three main aspects • Screening • Surveillance • Intervention • Pharmacological • Endoscopic • Surgical
Barrett’s Esophagus (BE) Screening (1) • Screening the general population with GERD • NOT recommended • Not enough evidence of benefit • 40% with esophageal adenocarcinoma have no preceding history of chronic GERD symptoms • Cost-ineffective, given the: • High prevalence of GERD (20% of US pop = GERD weekly) • Low incidence of esophageal adenocarcinoma
Barrett’s Esophagus (BE)Screening (2) • Targeted screening • Screening populations with high-risk factors • What’s recommended: • AGA (2011):Chronic GERD + ≥ 1 risk factor: • age 50 years or older • male sex • white race • hiatal hernia • elevated body mass index • intra-abdominal distribution of body fat • Tobacco use
Barrett’s Esophagus (BE)Surveillance • Regularly monitoring those with an established diagnosis of BE to detect progression and complications • Evidence does suggest endoscopic surveillance, with proper biopsy protocols, decreases mortality through earlier detection of treatable cancers • The more advanced the histology (i.e. low, high grade dysplasia), the more frequently surveillance is performed
Barrett’s Esophagus (BE) Intervention (1) • Pharmacological Chemoprevention • Proton pump inhibitors (PPIs) • Mostly indirect evidence • Acid damages DNA, proliferation, apoptosis • Some evidence of inverse relationship between long-term PPI therapy and incidence of dysplasia and adenocarcinoma in BE • Generally evidence is lacking that acid suppression prevents, causes regression of, or prevents progression of BE into esophageal adenocarcinoma • At least a daily PPI is administered • Therapeutic goal: minimum effective dose to achieve control of GERD symptoms and heal reflux esophagitis
Barrett’s Esophagus (BE) Intervention (2) • Non-steroidal anti-inflammatory drugs (including aspirin) • proliferation, apoptosis, angiogenesis • Some epidemiological studies have shown risk of adenoCA • However, risk of bleeding and cardiovascular side effects • Recommend using ASA in patients with cardiovascular risk factors, but not for BE alone • Anti-reflux surgery? (i.e. laparoscopic fundoplication) • No evidence it is more effective at preventing CA than medical therapy
Barrett’s Esophagus (BE) Intervention (3) • Endoscopic/Surgical • Indication: BE with high grade dysplasia • Choice of intervention dependent on local expertise, patient age, co-morbidities and patient preference
Barrett’s Esophagus (BE) Intervention (4) • Surgery - Esophagectomy • Historically, gold standard treatment of BE with high grade dysplasia • Advantage - curative • Disadvantages: • 2.5 – 20% mortality rate (depending on volume of center) • High morbidity (32% complication rate) • Dysphagia, early satiety, loss of appetite, fatigue • Most cancers detected in presence of high grade dysplasia are early stage with low risk of metastases (4%) • Less invasive endoscopic treatments are also now available • Bennett et al. (2012) – Consensus statement for HGD in BE • “Endoscopic treatment should be preferred over surgical treatment for management of most patients with HGD in BE”
Barrett’s Esophagus (BE) Intervention (6) • Advanced Endoscopic techniques • Performed through EGD to: • eliminate dysplasia • eliminate Barrett’s mucosa • prevent development of esophageal adenocarcinoma • Achieve reversion to normal squamous epithelium • i.e. Endoscopic Mucosal Resection (EMR)*, Radiofrequency Ablation (RFA)*, Cryotherapy, Photodynamic Therapy (PDT), Thermal Ablation, Endoscopic Submucosal Dissection (ESD) • Some have shown incredible promise • Shaheen et al. (2009): RFA eradicated dysplasia in 90.5% with low grade dysplasia, 81% with high grade dysplasia and 77.4% had complete BE eradication
Barrett’s Esophagus (BE) Intervention (7) Endoscopic Mucosal Resection Radiofrequency Ablation
Case 1 (cont’d) • EGD is performed and reveals columnar-appearing epithelium above the GEJ. Biopsies confirm BE with low grade dysplasia • Repeat endoscopy 6 months later confirms the same • He is placed on a PPI daily and is advised to return yearly for EGD surveillance
Case 2 (1) • Patient, unfortunately, does not return for follow-up • 10 years later he is re-referred for progressive, new onset solid food dysphagia, weight loss and anorexia • Bloodwork reveals a microcytic anemia with low ferritin
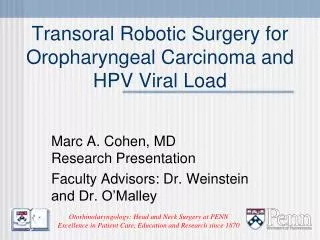
Esophageal Cancer • Two main types: • Adenocarcinoma • Squamous cell carcinoma • 1960’s • 90% of esophageal CA = squamous cell carcinoma • Over last 3 decades • incidence of esophageal adenocarcinoma • incidence of squamous cell carcinoma
Esophageal CancerEpidemiology Squamous Cell Carcinoma Adenocarcinoma Incidence in US: 2.5/100,000 Highest among whites Males > females (8:1) • Highest incidence: Asia, Africa, Iran • 1.4 – 140/100,000 • Incidence in US: 3-4/100,000 • Highest among african-americans (28.6/100,000) • Low incidence areas • More common in males • Generally not gender specific
Esophageal CancerRisk Factors Squamous Cell Carcinoma Adenocarcinoma GERD However, > 50% have no history of symptomatic reflux Smoking Obesity Drugs: LES pressure: Anti-cholinergics, beta blockers, benzodiazepines Oral bisphosphonates Diet: fruits, vegetables, fiber cholesterol, animal protein • Smoking • Alcohol • Diet • fruits, vegetables, selenium, zinc, folate • N-nitrosos compounds – pickled vegetables, betel nut • hot foods/beverages • Pre-existing esophageal disorders • Achalasia, caustic injury, HPV, tylosis, previous aerodigestive squamous cell cancer • Drugs: bisphosphonates 90%
Esophageal CancerClinical Manifestations • Age > 50 • Progressive solid food dysphagia • Unintentional weight loss • Anorexia • Retrosternal discomfort • Iron deficiency anemia • Advanced disease: • Sialorrhea, hoarseness, aspiration pneumonia, UGI hemorrhage • 40% - NO GERD symptoms Malignancy until proven otherwise
Diagnosis • Upper Endoscopy + biopsies • Radiological studies • Only adjunctive • Barium Swallow • CT scan
DiagnosisEGD • Early • Superficial plaques, nodules, ulcerations • Advanced • Strictures, ulcerations, circumferential mass