Download
1 / 8
80 likes | 441 Views
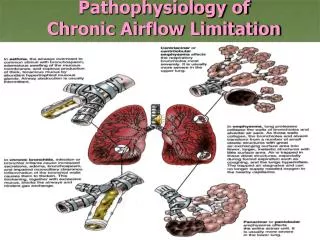
Pathophysiology of Chronic Airflow Limitation. Chronic Obstructive Lung Disease Emphysema. Abnormal permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis Risk Factors : Cigarette Smoking

E N D
Chronic Obstructive Lung Disease Emphysema • Abnormal permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis • Risk Factors: • Cigarette Smoking • Irritation - > 4,000 chemicals inhaled • Hyperplasia – reduces airway diameter • Abnormal dilatation of distal airspaces • Destruction of alveolar walls
Chronic Obstructive Lung Disease Emphysema • Risk Factors (cont’d): • Recurring respiratory tract infections • H. flu, Strep pneumoniae, Moraxella catarrhalis • Heredity – alpha 1 –Antitrypsin (ATT) deficiency • Accounts for <1% of COPD in US • AAT is a serum protein produced by the liver and normally found in the lungs • IV or nebulized AAT (Prolastin) slows COPD progression • Aging – Changes in lung structure • Gradual loss of elastic recoil – thin alveolar wall – thoracic cage changes from osteoporosis & calcification
Interferences with VentilationCollaborative Care Goals • Improve ventilation • Promote removal of secretions • Prevent complications & progression of symptoms • Promote patient comfort & participation in care • Improve quality of life as much as possible
Interferences with VentilationCollaborative Treatment • Patients are treated primarily as outpatients • Hospitalizations • Acute exacerbations • Complications • Respiratory failure, pneumonia, congestive heart failure
Interferences with VentilationCollaborative Management • Smoking cessation • Treatment of respiratory infections • Bronchodilator therapy • Beta2-adrenergic agonists • Anticholinergic agents • Long-acting theophylline • Corticosteroids • PEFR monitoring (peak expiratory flow rate) • Chest physiotherapy / Breathing exercises & retraining • Hydration 3L/day (unless contraindicated) • Rest - Progressive plan of exercise • Patient & family education • Influenza / Pneumovax immunization • Low flow oxygen rate (if indicated) • Pulmonary rehabilitation program