Download
1 / 22
230 likes | 645 Views
Spinal cord protection in surgery of descending thoracic aorta. Present by R1 康庭瑞. Case . 55 y/o male, HTN for 20+ years with regular medical control for 5 years Chronic dissecting aortic aneurysm type III noted for 5 years Left chest pain for 1 week Denied other systemic diseases

E N D
Spinal cord protection in surgery of descending thoracic aorta Present by R1康庭瑞
Case • 55 y/o male, HTN for 20+ years with regular medical control for 5 years • Chronic dissecting aortic aneurysm type III noted for 5 years • Left chest pain for 1 week • Denied other systemic diseases • Laboratory data: within normal range
Case • Normal screening spirometry • 2-D echocardiography: dilated aortic root(diameter 63mm) & LA, mild MR, good LV contractility • Planning: 1.Left post-lat thoracotomy 2. Femoral-femoral CPB 3. Hypothermia with circulation arrest and retrograde cerebral perfusion via high CVP 18~20mmHg by femoral artery perfusion and partial clamp of venous drain tube 4. Restore proximal aorta perfusion after proximal anastomosis through graft cannulation 5. Open distal anastomosis
Case • Cooling to 16℃ • Partial bypass: 3hr25min • Total bypass: 2hr30min • Aortic cross clamp: ?min • Circulatory arrest: 20min • Double lumen single-lumen ET tube ICU weaning and extubation on post-op day 3 without major complications
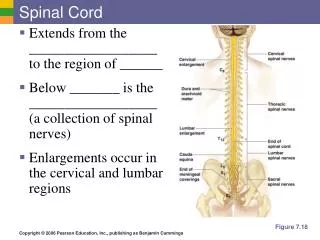
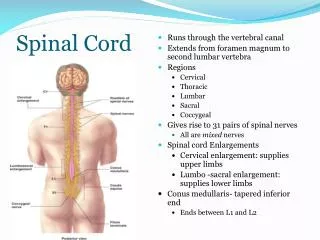
Consequences of aortic cross-clamping • Spinal cord ischemia • Vascular anatomy: single ant. spinal a. from vertebral a.supply ant. 2/3 of spinal cord; pair of post. spinal a. from post. cerebellar a.supply remainder of spinal cord • Spinal cord perfusion from: vertebral, deep cervical, intercostal, and lumbar a.radicular a. • The largest radicular a. (artery of Adamkiewicz): origin from T9~12 intercostal a. supply the majority of blood to the lower 2/3 of the spinal cord
Spinal cord ischemia • Paraplegia and paraparesis: major cause of morbidity and mortality after extensive TAAA repair • Incidence: 2~40%, depending on the site and the degree of aortic lesion, with/without dissection (2-fold), cross-clamp duration (less than 30min), ligation of the artery of Adamkiewicz, elevation in CSF pressure, reperfusion injury, perioperative hyperglycemia
Spinal cord perfusion pressure • CSF pressure increases during aortic clamping “spinal cord compartment syndrome” • Reduction of CSF pressure improves SCPP • Lumbar drains • Combined with distal aortic perfusion
Result • CSF pressure was maintained at 10mmHg or less • 148 nonemergent patients who received simple cross-clamping • 105 with combined adjuncts, 43 with or without the addition of a single adjunct • 0.9% vs 7% (p<0.04)
Result • 2.6% vs 13.0% • Reduced immediate deficits, particularly paraplegia • Infrequent delayed neurologic deficits in both groups • The longer the ischemic time were, the greater the benefit afforded with CSFD
Conclusions • Significantly reduced the rate of neurologic deficit during nonemergent repair of descending thoracic aortic aneurysms • The recently reports had convinced most surgeons of the benefit of CSF drainage in descending thoracic aortic aneurysm
Other adjuncts • Selective cooling spinal cord via lavage of the epidural space: regional hypothemic (26 ℃) protection of at-risk thoracolumbar cord • Corticosteroid, thiopental, NMDA antagonist, papaverine
Complications of lumbar drainage after TAAA repair • Postoperative lower extremity neurologic deficit: result of thromboembolic or delayed ischemic complication or resulting from lumbar drainage • Intradural hematoma: 3.2% in this study • CT, MRI
Hypothermic cardiopulmonary bypass and circulatory arrest • Methylprednisone and thiopental are given during the period of cooling to 15℃ • Circulatory arrest intervals: mean, 38min • Postoperative neurologic injury: 2.7% • Conclusion: hypothermic circulatory arrest offers certain advantages over other techniques and using of other adjunctive measures is not necessary
References • Hypothermic cardiopulmonary bypass and circulatory arrest for operations on the descending thoracic and thoraco-abdominal aorta. Annals of thoracic surgery.74(5):S1885-7,2002 Nov. • Cerebrospinal fluid drainage reduces paraplegia after thoracoabdominal aortic aneurysm repair: results of a randomized clinical trial. Journal of vascular surgery.35(4):631-9,2002 Apr. • Thoracoabdominal aneurysm repair: results with 337 operations performed over a 15-year interval. Annals of surgery.236(4):471-9,2002 Oct. • Complications of lumbar drainage after thoracoabdominal aortic aneurysm repair. Journal of vascular surgery.34(4):623-7,2001 Oct.