Download

1 / 64
640 likes | 798 Views
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE. Department of Internal Medicine and Gastroenterology University of Bologna L. Bolondi, L. Rasciti. Caso clinico. Donna di 56 anni, sposata con 3 figli, in menopausa da 5 anni.

E N D
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Department of Internal Medicine and GastroenterologyUniversity of BolognaL. Bolondi, L. Rasciti
Caso clinico • Donna di 56 anni, sposata con 3 figli, in menopausa da 5 anni. • Si accorge, guardandosi allo specchio, di lieve asimmetria della circonferenza del collo (modica tumefazione a sin); • Il medico palpa una formazione nodulare, di consistenza parenchimatosa, non dolente, verosimilmente riferibile al lobo tiroideo sin. Non rileva linfoadenopatie.
Caso clinico • Funzione tiroidea (FT3, FT4, TSH) nella norma • Autoanticorpi (anti TG, antimicrosomiali) nella norma • Emocromocitometrico, GOT, GPT, Azotemia, Glicemia, Protidemia totale ed elettroforesi, VES, Es; urine nella norma • Viene inviata per esame ecografico
NODULO ISOECOGENO CON AREA LIQUIDA INTERNA. AL DOPPLER SEGNI DI VASCOLARIZZAZIONE PERIFERICA
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Key concepts • Thyroid nodules are the most common endocrine disorder, they can be detected in an otherwise normal gland, especially in iodine-deficient areas. The frequency of thyroid nodules increases throughout life. • Single nodules are about four times more common in women thanin men.
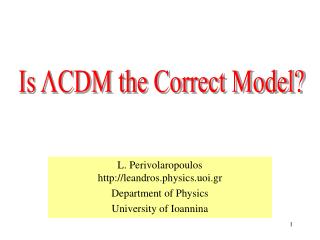
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Key concepts • Nodules are 10 times more frequent, in comparison to palpation, when the gland is examined at autopsy, during surgery, orby ultrasonography. Prevalence of palpable thyroid nodules detected at autopsy or by ultrasonography (solid circle) or by palpation (open square) in subjects without radiation exposure or known thyroid disease. E. Mazzaferri, NEJM 1993
Small (<5mm) non palpable thyroid nodule in the left lobe (occasional finding)
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Key concepts • Less than 1% of thyroid nodules detected at US prove to be malignant. • Less than 5% of solitary nodules detected at US are malignant. • A significant number of elderly patients have clinically silent thyroid cancers: up to 35% of thyroid glands at autopsy contain tiny (<1.0 cm), clinically unimportant papillary carcinomas. • Among nodules removed surgically, an estimated 42 to 77 % are non-neoplastic colloid nodules, 15 to 40 % are adenomas, and 8 to 17 % are carcinomas.
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE CLASSIFICATION OF THYROID NODULES Benign Nodules • Hyperplastic (colloid) nodule within goiter • Follicular Adenoma • Colloid variant • Hurthle cell variant • Papillary Adenoma (suspect for malignancy) • Teratoma
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE • Hyperplastic and Colloid (adenomatous) nodules are the dominant type of nodules, and can be single or multiple. • Most are hypofunctioning and incompletely encapsulated. Cytologic studies usually reveal abundant colloid and benignfollicular cells, but hemorrhagic nodules or highlycellular aspirates may be difficult to differentiate from follicular cancer.
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE • A diagnosis of a follicular or Hürthle cell tumor requires further evaluation and management, since the cytologic features of benign follicular or Hürthle cell tumors and low-grade follicular or Hürthle cell cancer are similar. • Benign from malignant nodules can only be distinguished by the presence or absence of capsular or vascular invasion on histologic examination of surgical specimens. • Follicular and Hürthle cell tumors have respectively a malignancy rate of 10% to 20%, that cannot generally be assessed adequately at FNAB .
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Malignant Nodules • Papillary Carcinoma (75-85%) • Pure papillary • Mixed papillary and follicular carcinoma • Follicular Carcinoma (20-25%) • Malignant adenoma • Hurthle cell carcinoma or oxyphil carcinoma • Clear-cell carcinoma • Medullary Carcinoma (5%) • Anaplastic Carcinoma (<5%) • Lymphoma • Metastatic tumor
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Nodules with sonographic apparence of cysts • Fifteen to 25 percent of all thyroid nodules are cystic. • High-resolution ultrasound has shown that most of the nodules initially considered to be cystic are complex lesions (solid-cystic). • Up to 15 percent are necrotic papillarycancers, and about 30 percent are hemorrhagic adenomas.
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Dectection of thyroid nodules • By chance during routine physical examination • By chance during US of the neck performed for other problem (i.e. carotid arteries, lymphnodes etc.) • In symptomatic patiens: local pain tenderness swelling dysphagia dysphonia hoarseness
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Clinical challenge: to identify which nodules are malignant • History and physical examination • Laboratory evaluation • Radionuclide scanning • Ultrasonography • FNA biopsy • UG-FNA biopsy
Benign Family history of benign thyroid nodule or goiter or autoimmune thyroid disease. Symptoms of hypothyroidism or hyperthyroidism. Pain or tenderness associated with the nodule. These factors do not exclude the presence of thyroid cancer. Malignant A family history of medullary or papillarythyroid cancer or of familial polyposis (Gardner's syndrome). Age—the young (<20 years old) and the old (>70 years old) have the highest incidence of thyroid cancer. Rapid tumorgrowth. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Clinical elements for differential diagnosis
Benign Soft, smooth, mobile nodule. Multinodular goiter without a dominant nodule. These factors do not exclude the presence of thyroid cancer. Malignant Gender—the proportion of nodules that are malignant in males is double that in females. Nodule plus dysphagia or hoarseness. Firm, hard, irregular, and fixed nodule. Presence of cervical lymphadenopathy. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Clinical elements for differential diagnosis
Malignant History of external neck irradiation during childhood or adolescence (this factor also increases the incidence of nonmalignant thyroid nodular disease) or exposure to nuclear fallout. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Clinical elements for differential diagnosis Benign
Laboratory evaluation In patients with a thyroid nodule, a sensitive thyroid stimulating hormone (TSH) assay should be done, at a minimum, to determine the presence of hyperthyroidism or hypothyroidism. Serumcalcitonin should be measured when medullary thyroid carcinoma or MEN IIis suspected. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
Radionuclide scanning Aim: to identify hyperfunctioning nodules that are almost always benign. Limits: lack of differentiating criteria for hypofunctioning nodules Not all patients with thyroid nodules require nuclear imaging. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE Ultrasonography • Widespread use of ultrasound for examining any neck pathology has resulted in frequent recognition of thyroid nodules, that are too small to be palpated on clinical examination. • Usually, such nodules are < 1cm in largest diameter, they are typically asymptomatic, and are not associated with lymph nodes or other suggestions of malignancy. • Often incidentally found, such nodules produce a problem because of the difficulty in achieving a specific diagnosis, which is desired by the patient.
Ultrasonography In a recent metanalysis (Ann Intern Med, 126:226-31, 1997.), the risk for malignancy in US incidentalomas ranged betwen 0.45% and 13%. Large malignant nodules have beenreported to be missed by palpation.The greatest size of malignant non palpable nodules was 2.1 cm. Theexistence of these nodules, detected by US exploration, suggeststhat a simple follow-up neck palpation, may not be the safest management strategy. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
Ultrasonography Currently no ultrasound criteria can distinguish benign from malignant thyroid nodules. However some features are suggestive for malignancy: Microcalcification Irregular or microlobulated margin Hypoechogenicity Intranodular blood flow pattern CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
NODULO ISOECOGENO CON AREA LIQUIDA INTERNA. AL DOPPLER SEGNI DI VASCOLARIZZAZIONE PERIFERICA
TIROIDE: NODULO PARZIALMENTE CISTICO CON CALCIFICAZIONI
PAPILLARY CARCINOMA Intranodular Vascularization
FNA biopsy FNAB has become the initial test, after clinical and/or US examination, because it is safe and inexpensive and leadsto a better selection of patients for surgery. FNAB is now believed to be the most effective method available for distinguishing between benign and malignant thyroid nodules. In this setting the FNAB sensitivity varies from 68 to 98% (mean, 83%) and specificity varies from 72 to 100% (mean, 92%). CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
FNA biopsy Provided that an adequate specimen is obtained, three cytologicresults are possible: benign, malignant, and indeterminate (orsuspicious) findings. A major problem diminishing the potential benefit of FNAB is the unskilled physician performing the biopsy or the inexperienced cytopathologist interpreting the specimens. Even in skilled hands, however, approximately 10% of biopsy findings are nondiagnostic. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
FNA biopsy Repeated FNAB may be appropriate under several circumstances as follows: (1) when the lesion continues to enlarge; (2) when new clinical features develop that suggest possible malignancy; (3) when the previous cytologic diagnosis was indeterminate, or (4) when there is insufficient material for cytologic diagnosis. Routine repetitive FNAB of lesions that were previously shown to be benign is rarely indicated. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
UG-FNA biopsy Ultrasound-guided FNAB (UG-FNAB) has emerged as an alternative to conventional FNAB for the diagnostic evaluation of nonpalpable nodules and for the repeat evaluation of nodules with previous nondiagnostic FNAB. It is also an excellent method for the evaluation of complex nodules by precisely positioning the needle in the solid portion of these nodules. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
FNAB OF SOLID THYROID NODULE The arrow points to the needle
UG-FNA biopsy In the literature, the sensitivity and specificity of UG-FNAB amounted to 79% and 85%, respectively. UG-FNAB is possible for lesions smaller than 1 cm in size, but considering the probable benign nature of most of such lesions, a common alternative course is "observe" such lesions periodically. Due to the high prevalence of USthyroid nodules, a systematic UG-FNAB performed on all nonpalpablenodules is not advisable. CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE
CLINICAL AND SONOGRAFIC APPROACH TO THE THYROID NODULE PALPABLE THYROID NODULE ULTRASONOGRAPHY NOT PALPABLE THYROID NODULE SINGLE NODULE 1 cm or DOMINANT NODULE INCREASED RISK YES NO NO INCREASED RISK YES NO YES TSH < 0.03 CYST YES NO NO US SIGNS FOR MALIGNANCY YES NO YES FNAB UG-FNAB COLD NODULE NO YES HOT NODULE NO DIAGNOSTIC YES NO YES BENIGN NO INCREASED RISK TREATMENT SUSPICIOUS TSH < 0.03 TSH > 4.5 YES YES FOLLICULAR LESION NO SURGERY CANCER FOLLOW UP US and LAB