Download

1 / 28
300 likes | 685 Views
Nephropathology Slide seminar case 3. Granulomatous interstitial nephritis. Vazquez Martul Eduardo.MD Coruña .Spain. Painting. Uroscopia. David Teniers, XVII CENTURY Art´s Museum. Brussels. Case history

E N D
NephropathologySlide seminar case 3. Granulomatous interstitial nephritis Vazquez Martul Eduardo.MDCoruña .Spain
Painting. Uroscopia. David Teniers, XVII CENTURYArt´s Museum. Brussels Case history A male 59 years old with previous history of pulmonary disease with diagnostic of sarcoidosis three years before (dec 2005), with mediastinic and interstitial pulmonary affectation. No history of renal dysfunction was detected at that moment.The Crp was 1.3 mg/dl . Corticoid treatment was supplied with improvement of lung symptoms. November 2009, he was hospitalized because it was detected in a routine analysis a deterioration of renal function with a Crp 3.4mg/dl. The patient only reported malaise without urinary symptoms since one month before. No fever, thoracic, lumbar pain or dermatologic alteration was detected. The BT was 120/80. He denied intake of any antibiotic or anti-inflammatory treatment.Hemogramme: erythrocites: 4.56,leucocyte:6.130, lymphocyte 21%, monocyte 11%, neutrophil 3.780, glucose 90mg, urea 977, total bilirrubin 0.6 mg., uric acid 8 mg, calcium 11, P 3.9, Na 138, K 4.6 urea 80 mg, cholesterol 182mg, triglyceride 180 mg. Urine analysis: sediment normal, no hematuria., no proteinuria.Density 1.010.
Preliminary Diagnostic guide-lines • ANCA DISEASE. • Granulomatosis with polyangiitis • ANTI-GBM GLOMERULONEPHRITIS • Tubulointerstitial disease; SARCOIDOSIS 59 year old male With mediastinic and lung nodular affectation Rapid deterioration of renal function A kidney biopsy was indicated
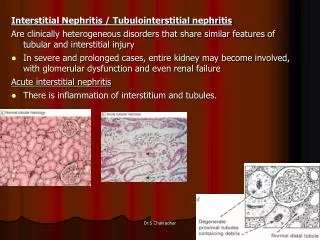
Granulomatous nodules Tubular destruction
Lymphoide cellular infiltration Eosinoph leucocytes Histiocytes
HISTOPATHOLOGIC DIAGNOSIS • GRANULOMATOUSTUBULOINTERSTITIAL • NEPHRITIS • EPITHELIOID GRANULOMAS COMPATIBLE WITH SARCOIDOSIS.
RENAL GRANULOMATOSES • DRUG INDUCED • INFECTION :TUBERCULOSIS • VASCULITIDES • SARCOIDOSIS
Clinical and laboratory features at presentation in patients with AIN Features Acute renal failure 100% Acute renal failure requiring dialysis 40% Arthralgias 45% Fever 36% Skin rash 22% Eosinophilia (4500 eosinophils per mm3) 35% Microhematuria 67% Gross hematuria 5% Leukocyturia 82% Non-nephrotic proteinuria 93% Nephrotic-range proteinuria 2.5% Complete nephrotic syndrome 0.8% From Praga M, Gonzalez E. Acute interstitial nephritis Kidney Int 2010;77:956
Table 1 | Etiology of biopsy-proven AIN • Drugs (47.5% of AIN) Antibiotics: ampicillin,cephalosporins, • ciprofloxacin, cloxacillin, methicillin, penicillin, • rifampicin, sulfonamides, vancomycin. • NSAIDs • Other: allopurinol, acyclovir, famotidine, • furosemide, omeprazole, phenytoin • Infections (5–10%) • Bacteria: Brucella, Campylobacter, Escherichia coli, Legionella, Salmonella, Streptococcus, • Staphylococcus, Yersinia • . Viruses: cytomegalovirus, Epstein–Barr, • hantavirus, human immunodeficiency virus, polyomavirus • Other: Leptospira, Mycobacterium tuberculosis, • Mycoplasma, Rickettsia, Schistosoma, Toxoplasma • Idiopathic (5–10%) • Anti-TBM • TINU • Associated with systemic diseases (10–15%) • Sarcoidosis, Sjogren, systemic lupus erythematosus. • Abbreviations: AIN, acute interstitial nephritis; NSAID, nonsteroidal anti-inflammatory • drug; TBM, tubular basement membrane; TINU, tubulointerstitial nephritis and From Praga M, Gonzalez E. Acute interstitial nephritis Kidney Int 2010;77:956
Sarcoidosis : Differential diagnostic Tuberculosis ¡¡¡Attention!!! fever can be present in sarcoidosis Zhiel-Nielsen
Granulomatous Interstitial nephritis: differential diagnosis • Cases associted with lymphoid infiltration and uveitis TINU syndrome • Cases without granuloma
Granulomatous vasculitis Renalsarcoidosis presenting as acute kidney injury with granulomatous interstitial nephritis and vasculitis. Agrawal V, Crisi GM, D'Agati VD, Freda BJ. Am J Kidney Dis. 2012 Feb;59(2):303-8. Epub 2011 Dec 15. Sarcoidosis and Rapid Progresive Renal failure Berner Bet al. Med klin 1999,94.690
Acute renal failure and Interstitial nephritis: differential diagnosis Giant cell: DIFFERENTIAL DIAGNOSIS kappa Light Chain deposit disease
Granulomatous interstitial nephritis is a rare condition whose pathogenesis is poorly understood. 0.5- 1.5 THE RENAL BIOPSIES Of 203 renal biopsies performed between 1974 to 1994 in which interstitial nephritis was the predominant change, granulomata occurred in 12. Sarcoidosis accounted for granulomatous inflammation in three patients Hum Pathol. 1995 Dec;26(12):1347-53. Granulomatous interstitial nephritis. Viero RM, Cavallo T. In our experience since 1978 up to now (3.000 kidney biosies) only two cases
Granulomatous interstitial nephritis: A retrospective study of 44 cases] . Pasquet F, Chauffer M, Karkowski L, Debourdeau P, Mc Grégor B, Labeeuw M, Laville M, Pavic M. Rev Med Interne. 2010 Oct;31(10):670-6. Granulomatous interstitial nephritis (GIN) are identified in 0.5 to 1,3% of all renal biopsies. 20% in prviously diagnosed sarcoide patients The study population included 25 men and 19 women with a mean age of 56 years Renal function wasseverely impaired (mean creatinine clearance 24mL/min) in 43 patients. Proteinuria was observed in 77% The most common diagnosis was sarcoidosis (25%, n = 11), followed by drug-induced GIN (9%, n = 4), tuberculosis (6,8%, n=3),
Renal sarcoidosis: clinical, laboratory, and histologic presentation and outcome in 47 patients. • Mahévas M, Lescure FX, Boffa JJ, Delastour V,et al. • Medicine (Baltimore). 2009 Mar;88(2):98-106 French Sarcoidosis Group. (30 male/17 female, M/F ratio: 1.76). • Thirty-seven patients presented noncaseating granulomatous interstitial nephritis • and 10 presented interstitial nephritis without granulomas. • All but one presented ARF • Fifteen of 47 (32%) patients had hypercalcemia (>2.75 mmol/L).
SARCOIDOSIS AND KIDNEY INTERSTITIAL GRANULOMATOUS NEPHRITIS HYPERCALCEMIE (2-20%) ARF TINU syndrome associated Bilateral kidney pseudotumor Vicente A, Acebal Blanco MM. Arch Esp Urol. 2012 Jul;65(6):629-. Nefrocalcinosis Nephrolitiasis (1-14%) • GLOMERULAR • GN membranosa • GN membrano- • Proliferativa • GN mesangial IgA • Nefropatía por • cambios mínimos • GEFS • Vasculitis sistemica proteinuria CKD
CD68 SARCOIDOSIS Pathogenesis?? CD68 CD5 CD5 CD20
PATHOGENESIS: SARCOIDOSIS II GENES:DRB1/DQB1 Lower levels TGF-beta1 DPB1 gene calcitrol FIBROSIS hypercalcemis RESOLUTION Chronic KD Sato H,Woodhead FA,AhmadT et al. Hum Mol Genet, 2010.19.4100
General concepts and summary • Sarcoidosis is a multisystemic disease of unknown etiology. • It is characterized by the presence of non- caseating epitelioid granulomas in various organs. Renal disease is common in previously sistemic sarcoidosis up to 20% but very infrequent in routine biopsies (less 1.5%) • It is necessary to mark out that GIN is not pathognomonic of sarcoidosis: being also present in drug reactions, mycobacterial and fungal infections and in granulomatosis vasculitis. • Most renal disease related to sarcoidosis is due to hypercalciuria and nephrocalcinosis is the most common disease. • A good response to treatment with corticosteroids • End-stage renal disease from sarcoidosis is usually due to hypercalcemia, renal stones and obstructive uropathy • Cases associated with vasculitis, lymphoid interstitial nphritis (TINU S) • The association between any form of glomerulonephritis and sarcoidosis is fortuitous • Postransplant recurrence is observed in 27%.
Selected References • Granulomatous interstitial nephritis. Vieiro RM, Cavallo T. • Human Pathol. 1995,26: 1347-53 • Granulomatous interstitial nephritis in an extrapulmonary sarcoidosis • Utas C, and al.Clin Nephrol 1.999,25:252 • Renal disease in sarcoidosis. Curhan GC edit. Burton D Rose and G. Rizzato.2012 www.uptodate. • Frequency of kidney disease in chronic sarcoidosis. • Bergner R, Hoffmann M, Waldherr R, Uppenkamp M. • Sarcoidosis Vasc Diffuse Lung Dis. 2003 Jun;20(2):126-32. • Renal failure in sarcoidosis]. • Sadek BH, Sqalli Z, Al Hamany Z, Benamar L, Bayahia R, Ouzeddoun N. • Rev Pneumol Clin. 2011 Dec;67(6):342-6. • Granulomatous interstitial nepritis.- Nicola Joss et al.,CJASN 2007 ,2:222-230 • 18 cases: 5 associated with sarcoidosis. • Granulomatous interstitial nephritis: A retrospective study of 44 cases] • Pasquet F, Chauffer M, Karkowski L, Debourdeau P, Mc Grégor B, Labeeuw M, Laville M, Pavic M. • Rev Med Interne. 2010 Oct;31(10):670-6. • . • Renal sarcoidosis: clinical, laboratory, and histologic presentation and outcome • in 47 patients.Mahévas M, Lescure FX, Boffa JJ, Delastour V,et al. • Medicine (Baltimore). 2009 Mar;88(2):98-106