Download
1 / 28
280 likes | 421 Views
Case Study Of A Primary Care Accountable Care Organization. David R. West, PhD Robert Phillips, MD, MSPH AHRQ Task Order: SNOCAP-USA (University of Colorado) HHSA290200710008 Dr. David Lanier: Task Order Officer September 28, 2010. DISCLOSURE I have no financial relationships to disclose

E N D
Case Study OfA Primary Care Accountable Care Organization David R. West, PhD Robert Phillips, MD, MSPH AHRQ Task Order: SNOCAP-USA (University of Colorado) HHSA290200710008 Dr. David Lanier: Task Order Officer September 28, 2010
DISCLOSURE I have no financial relationships to disclose And I will not discuss off label use and/or investigational use in my presentation
Project Team From the Robert Graham Center • Robert Phillips, MD, MSPH: Task Order Leader • Svetlana Bronnikov, MS • Stephen Petterson, PhD • Bridget Teevan, MS, MPH From the University of Colorado • Maribel Cifuentes, RN
What Can We Learn From a “Mature” PCMH? • Aim 1: Determine: How A PCMH developed their model • Aim 2: Determine if the PCMH improved processes of care and outcomes • Aim 3: Determine the incremental in-practice expenses (reduced to a pm/pm) required to operate the patient-centered medical home
Mixed Methods Approach Qualitative Analysis • 58 Key Informant Interviews (Executives, Clinicians, Administrative and Finance staff, Patients Quantitative Analysis • Collection/analysis of reported process and outcome indicators • Analysis of WellMed vs. matched CMS data (Parts A and B): Controls for Ischemic Heart Disease (IHD), Chronic Obstructive Pulmonary Disease (COPD), and Type 2 Diabetes Mellitus (DM)
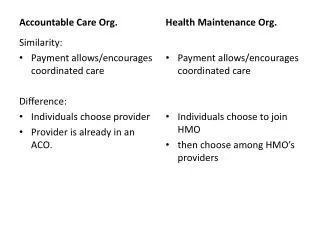
WellMed As A Case Study (in progress) • Have been providing primary care services for 20years in their community • Accepts full risk capitation for most services (primary care, specialist care, physician, inpatient hospital, outpatient hospital, etc.) • Documented use of a patient-centered continuous quality improvement approach including social services, prevention, and active disease management protocols • Availability of electronic health data for analysis
PCMH PCMH PCMH PCMH PCMH PCMH WellMed Accountable Care Organization Hospital Specialist Social Services Transportation
Practice setting • Lots of space • In primary care trend is downsizing footprint • Big community space for exercise classes, computer classes, nutrition/cooking classes • Podiatry, Rheumatology, Dermatology rotate through • Free orthopedic shoes fitted onsite
Teams With Defined Roles • Med Assistants do most data entry • Health Coaches • Call patients next day to reinforce care plan • Meet with patients (clinic, home, phone) to do behavior change, mental health, care plan • Disease Mgmt program for COPD, DM, CHF, CAD—manage most fragile, high cost patients intensely
Teams Continued… • Inpatient • Their own case managers and hospitalists (their culture, their plan) • Interventions for specific conditions—national award for model Knee Replacement protocol • Nursing home teams led by NPs for nursing homes (4 core)
Teams Continued… • Very low turnover compared to market • Grow their own—able MAs trained and mentored into higher roles • Starting an MA school • cut usual cost in half (more diversity) • Train to their model • Two week orientation for new physicians + pairing with best clinicians for shadowing and mentoring
Control of Dollars & Data • Data for all patients, all settings, all care • Very innovative population data array • Used to monitor quality • Identify, develop, evaluate interventions • Identify outliers; not keeping appointments, not filling prescriptions, increased utilization • Team bonuses based on quality improvement
PCMH TIMELINE 1190 Established with particular emphasis on Medicare population 1991 Strengthen and support primary care role in health care (e.g., support comprehensive care approach including hospital and nursing home care, work on team based chronic disease care 1993 Begin benefits review process to add benefits that remove patient barriers to essential care – this eventually includes transportation help, paid health maintenance visits, expanded medication coverage for essential medications, expanded eye care, expanded dental benefits, expanded hearing aid benefits 1996 Same day appointments available in medical offices 1998 Regularly track patient satisfaction 1999 Starts disease management division
2001 Installs EHR including electronic prescribing2002 Add clinical decision support system along with improved registry functions2003 Transform disease management to health coach concept- patient centered and available to all patients 2006 Web access to patient level data for treating specialists2006 Portable “EHR” system given to patients to improve data transfer to other care providers2008 Transitions “Health Coach” function from a centralized approach to primary care office based approach and begin transition to expanded team based chronic care model2008 Web access for medical data for patients
Trends in rates of health screening & meeting chronic disease targets
Qualitative Analysis Research Questions: • How did WellMed develop their level 3 PCMH model – the facilitators, barriers, key components, history and leadership? • How did the implementation of the WellMed model impact patient and provider satisfaction?
Qualitative Analysis Themes Patients identify five factors of the WellMed model as important to their satisfaction: • Personal relationship with a physician over time • Access, ease of making appointments • Being greeted cordially, technical competency, compassion, taking time to listen and explain information • Affordability… of medications, discounted prices, reasonable co-pays • Getting referrals, having people remember basic care (e.g. flu shots)
Qualitative Analysis Themes • Staff identify four factors of the WellMed organization that are important to their satisfaction: • Belief in what the company stands for and the sharing of values • Good compensation and bonuses • Leadership that listens and values employees • Opportunities for advancement
Qualitative Analysis Themes • The guiding principles from which the WellMed model was constructed and the way in which the model has evolved stem from and promote the 4 pillars of primary care • Easy access to first contact care • Comprehensive care – accountability for addressing large majority of personal healthcare needs. Includes the convenience of having majority of services under one roof • Coordination of care • Personal relationships over time • WellMed has acted on these primary care principles by using ACO methods
Qualitative Analysis Themes • 5 Key factors used to guide and implement the marriage of PCMH and ACO elements of the WellMed model • Use of economics as a driver for quality • Collaborating and coevolving with others that understand and buy-in to the model • Customer service is key to everything we do • Identify every day problems and implement common sense solutions – evolve solution as needed. “is there a way we can do this better and more efficiently” • We’re big on prevention
NEXT STEPS • Completing Qualitative Study • Completing matched cohort study (costs/outcomes of similar Medicare beneficiaries) • Completing financial/Business Model Review