Download
1 / 32
340 likes | 851 Views
Cervical Radiculopathy Following MVA. Case Study Ramsee Pagel, SPT Regis university Summer 2010. Objectives. The student will be able to understand the relationship between pathology and presentation of cervical radiculopathy following a MVA

E N D
Cervical Radiculopathy Following MVA Case Study Ramsee Pagel, SPT Regis university Summer 2010
Objectives The student will be able to understand the relationship between pathology and presentation of cervical radiculopathy following a MVA The student will examine and understand the current best evidence supporting physical therapy intervention for cervical radiculopathy. The student will be able to understand the examination, evaluation, and intervention for those patients who present with cervical radiculopathy following MVA.
Purpose To examine whether physical therapists are selecting interventions using an evidence based approach when treating patients who present with neck pain and radicular symptoms following trauma.
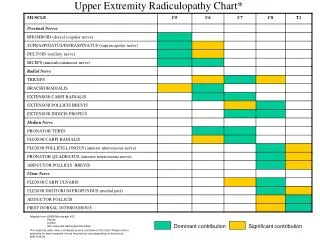
What we know… • Pathology • Nerve root compression, inflammation, or improper function • Radicular symptoms • Herniated disc • Degenerative changes in the spine • Other injuries (trauma) • Pt Presentation • Neck pain • Arm pain • Numbness and tingling in the UE • Pain will occur anywhere along the nerve root distribution
What we know… • Using the knowledge we have learned in our education up to this point: • Clinical Prediction Rule – Cervical Radiculopathy • (+) ULTT A • (+) Distraction • (+) Spurlings • Ipsilateral Cervical Rotation <65° • Wainner et al., SPINE, 2003.
History Pt is a 33 year old female who works as a Respiratory Therapist. Pt was referred to physical therapy following an MVA. Rx: Evaluate and Treat (4/20/2010) Dx: Levator scapulae syndrome with cervical strain and right SI joint strain s/p MVA. Treatment Dx: Decreased cervical AROM with right UE radicular symptoms and pelvic asymmetry with piriformis dysfunction.
History • PIPs: pain limiting reaching overhead and her abilities to lift and care for her three children. • At the time of initial examination, the patients stated that her low back pain was limiting most of her activities and the UE/Cervical spine symptoms were not as limiting. • Images (plain films) were taken following the accident and no abnormalites were noted. • A cervical MRI was also done after 10 PT visits • Mild disc herniation at C4-C5 with no signs of cord compression.
Patient Presentation PROM UE: WNL AROM UE: Bilateral shoulder flexion limited by 20 degrees secondary to pain AROM C-spine: flexion/extensionWNL, right rotation 65°, left rotation55° UE Strength: 4/5 throughout bilaterally with pain during testing Reflexes: Bilateral UE reflexes2+ throughout L UE Pain: 9/10 Neck Pain: 9/10 LBP:10/10 NDI: 44%severely disabled ODI: 40%moderately disabled
Cervical Special Tests • At initial examination: • (+) Sharp Purser • (+) Right Spurlings • (-) Left Spurlings • (+) Distraction • (-) ULTT Bilateral • Median • Ulnar • Radial
Differential Diagnosis • Cervical Radiculopathy • Fracture • Vertebral • Scapular • Humeral • Shoulder Impingement • Biceps Tendonitis/Bicep Tendon Rupture • Rotator cuff inflammation/rupture
Other Factors • Psychological • Frequent flashbacks • High anxiety • Little to no sleep • Fear about the inability to work and properly care for her 3 children • Pt was seeing a clinical psychologist 2x/month for counseling
Clinical Decision Making Using the patient identified problems, the initial intervention was directed towards the low back and pelvic asymmetry. Secondly, since the patient did not fall completely into any of the clinical prediction rules, cervical mechanical traction was not immediately initiated. Functional goals were set to decrease overall pain, improve mobility of the cervical and lumbar spine, and increase the patients overall function.
Response to Intervention • Pt reported 1/10 LBP following 10 treatment sessions • Interventions: • Pelvic MET • Core Stabilization Exercises • Lumbar Flexion Manipulations • Prone PA Thoracic Mobilizations • IFC with HP • Pt reported slight decrease in neck and arm pain after 10 visits • Interventions: • STM • Rotational MET • Sub-Occipital Release • Manual Distraction • Cervical Segmental Mobilizations • IFC with HP
Cervical Special Tests • After 10 visits: • (+) L Spurlings • (-) R Spulings • (+) Distraction • (+) Shoulder Abduction Test • (+) ULTT A • (-) Sharp Purser • R Rotation: 65° • L Rotation: 42° • NDI score 48% (severely disabled)
What the Evidence Says… • Treatment Based Classification System • Which category does the pt most match? • Were the interventions provided matched to that category? • At initial examination? • After 10 visits?
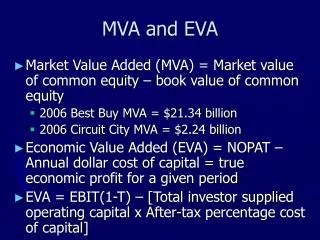
Treatment-Based Classification • Fritz, J. Brennan, G. Preliminary examination of a proposed treatment-based classification system for patients receiving physical therapy interventions for neck pain. Phys Ther, 2007. • Purposes of the study • Examine proposed treatment-based classification system by describing prevalence of subgroups in a sample of patients receiving PT for neck pain • Compare other characteristics of patients placed in these subgroups
Neck pain classification categories and matched interventions • Mobility • Mobilization/ Manipulation of cervical or thoracic spine • Strengthening exercises for the deep neck flexors (DNF) • Centralization • Mechanical or manual cervical traction • Cervical retraction exercise • Exercise and conditioning • Strengthening exercises for upper-quarter musculature • Strengthening exercises for neck/ DNF • Pain control • Cervical spine mobilization • Cervical range-of-motion exercises • Head Ache • Cervical spine manipulation/mobilization • Strengthening exercises for DNF • Strengthening exercises for upper-quarter musculature
Results • 297 patients with neck pain were evaluated • 274 were included in analysis • 113 (41.2%) patients received interventions that matched prespecified treatment components • 161 (58.8%) received nonmatched interventions • Patients receiving matched interventions showed greater changes in both NDI and pain rating scores. • Among patients receiving matched interventions, 72.5% achieved the minimal detectable change (MDC), whereas only 53.8% of patients receiving nonmatched interventions did so (p=.002).
Where do we go from here? • Using the treatment based classification system: • Initially, the pt fell mostly into the pain control category • After 10treatment sessions, the pt fell more into the centralization category
Matched Intervention- Mechanical Traction • Raney, N. et al. Development of a clinical prediction rule to identify patients with neck pain likely to benefit from cervical traction and exercise. Eur Spine J. 2009. • Parameters- Traction • Angle of pull: 24° flexion • On/off cycle: 60:20 • Initial pull: 10-12 pounds • Progressed per patient tolerance • Maximum pull: 40 pounds • Rest force: 50% of pull force • Total time: 15 minutes • Exercise protocol • DNF and Postural exercises (scapular squeezes)
Matched Intervention- Mechanical Traction • Clinical Prediction Rule- Success from mechanical traction and exercise • Patient reported peripheralization with lower cervical spine mobility testing • (+) ULTT A • (+) Distraction • (+) Shoulder Abduction Test • Age ≥ 55 • Likelihood of patient reported success • 5/5=100% • 4/5=94.8% • 3/5=79.2% Raney, N. Eur Spine J. 2009.
Matched Intervention • Mechanical Traction and Exercise • Initiated after 12 visits • Parameters: • Max pull 14 pounds • Total pull time 6 minutes • Intermittent 60:10
Intervention Progression • Traction pull was progressed after 4 sessions • Max pull16 pounds • Total pull time 6 minutes • Intermittent 60:10 • Pull was then progressed by 2 pounds each session per pt tolerance • Total pull time was also progressed by 2 min each session per pt tolerance • At the conclusion of CE II • Max pull24 pounds • Total pull time14 minutes • Intermittent 60:10
Exercise and Manual Therapy Interventions DNF10 x 10 sec TherabandRows blue band x 15 TherabandExtenstions blue band x 15 Scapular Squeezesx 20 Cervical rotation MET STM Manual Scalene Stretch Subocciptal Release Prone PA Thoracic Spine Mobilizations Cervical Segmental Mobilizations
So what can we expect?? • Cleland, J. et al. Predictors of short-term outcome in people with the clinical diagnosis of cervical radiculopathy. Phys Ther. 2007. • Purpose: to determine which factors noted at baseline evaluation can be predictive of short term outcome in patients with the clinical diagnosis of cervical radiculopathy. • Outcomes used: • NDI • NPRS • PSFS
So what can we expect?? • Results: • The study design did not allow for a cause and effect relationship to be established • The results suggest that mechanical traction, deep neck flexor strengthening, postural education, and manual therapy may be beneficial in the management of cervical radiculopathy • With 3 of the 4 treatment variables present the +LR=5.2 with the posttest probability of success =85%
Pt Presentation • On 7/2/2010 • VAS 3/10 neck • VAS 3/10 L UE • Pain is inconsistent and is much worse at night • Pain is still limiting her ability to perform ADL’s • NDI: 30% moderate disability • Pt states she is feeling much better but it is a slow process and she just wants to be able to be a mom with no pain again. • Pt continues to have 0-1/10 LBP
What could have been done differently?? • Utilized other outcome tools? • FABQ • PSFS • Reassessed more frequently? • Progressed traction more frequently using the published literature? • Pt tolerance/anxiety levels
Check For Understanding • 1. Which of the following is not a test included in the CPR for cervical radiculopathy? • A. Cervical Distraction • B. Craniocervical Flexion • C. Spurlings • D. ULTT A • 2. T/F: all patients will fall into a single category according to the treatment based classifications. • 3. T/F: there is evidence to support the use of mechanical traction, manual therapy, and exercise in the management of patients with cervical radiculopathy.
References Cleland, J. et al. Predictors of short-term outcome in people with the clinical diagnosis of cervical radiculopathy. Phys Ther. 2007. Fritz, J. Brennan, G. Preliminary examination of a proposed treatment-based classification system for patients receiving physical therapy interventions for neck pain. Phys Ther, 2007. Raney, N. et al. Development of a clinical prediction rule to identify patients with neck pain likely to benefit from cervical traction and exercise. Eur Spine J. 2009. Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison S. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine. 2003.