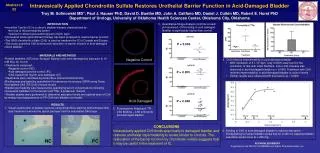
Interstitial Cystitis Painful Bladder Syndrome
Interstitial Cystitis Painful Bladder Syndrome. Hann-Chorng Kuo Department of Urology Buddhist Tzu Chi General Hospital Hualien. Interstitial cystitis. A syndrome of mystery in urology A diagnosis of exclusion

Interstitial Cystitis Painful Bladder Syndrome
E N D
Presentation Transcript
Interstitial CystitisPainful Bladder Syndrome Hann-Chorng Kuo Department of Urology Buddhist Tzu Chi General Hospital Hualien
Interstitial cystitis • A syndrome of mystery in urology • A diagnosis of exclusion • Triad diagnostic characteristics –Suprapubic pain at full bladder and relieved after voiding, with severe frequency and nocturia Sterile urine Characteristic cystoscopic findings
Diseases associated with IC • Allergies, autoimmune diseases, rheumatic disease,irritable bowel syndrome • A common pathophysiology mediated by immune, endocrine & neurologic dysfunction • Systemic lupus erythematosus • The role of mast cell (increase histamine release from bladder biopsies) in IC
Epidemiology of IC • In a survey of USA Nurse’s health Study, self-reported IC was 0.4% (357 in 91155 NHSI) and 1.4% (1354 in 993428 NHSII) • NIDDK criteria is too restrictive, about 60% excluded patients may have IC • The prevalence of IC was estimated to be 52 per 105 (NHSI) and 67 per 105
Possible pathogenesis of IC • Post-infection autoimmune process • Mast cell activation – inflammation, toxin, stress • Urothelial dysfunction – increased permeability of urothelium • Neurogenic inflammation – K diffusion- mast cell activation – upregulation of sensory fiber – release of neuropeptide (substance P) – neurogenic inflammation – pain in IC
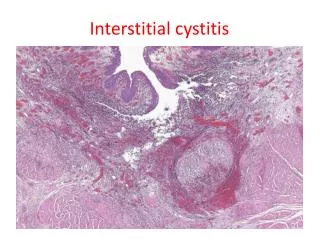
Characteristic cystoscopic findings after hydrodilatation • Classical IC – contracted bladder, Hunner ulcer • Early IC – glomerulation, petechial hemorrhage, mucosal fissure • Recent investigations revealed classical IC may be misleading, chronic IC may be more accurate to describe pathology
Interstitial cystitis • 1915 Hunner – an elusive ulcer after secondary bladder hydrodilation • 1949 Hand – Female tomale ratio 11:1 • 1975 Oravisto – incidence about 18/105 • 1978 Messing – Glomerulation after hydrodilatation • 1982 Larsen – mast cell quantitative assessment in IC • 1983 Parsons – a defect in bladder GAG layer • 1987 Holm-Bentzen – painful bladder syndrome • IC remains a syndrome of unknown etiology, difficult to diagnosis and treatment
IC patient accrual form –NIDDK 1987 automatic exclusion • Less than 18 years old • Benign or malignant bladder tumor • Irradiation cystitis • Tuberculous cystitis • Bacterial cystitis • Vaginitis • Cyclophosphamide cystitis • Symptomatic urethral diverticulum • Uterine, cervical, vaginal, or urethral cancer
IC patient accrual form-- automatic exclusion • Active herpes • Bladder or lower ureteral calculi • Waking frequency < 5/12 hours • Nocturia <2/night • Symptoms relieved by antibiotics, urinary antiseptics, analgesics • Involuntary detrusor contractions • Capacity > 400ml, no sensory urgency
IC patient accrual form-- automatic inclusions • Hunner’s ulcer • Positive factors – • Pain on bladder filling relieved by emptying • Pain (suprapubic, pelvic, urethral, vaginal, perineal) • Glomerulation on endoscopy • Decreased compliance on cystometry • Bladder distention by 80 cm water x 1 min, two positive factors are necessary
Cystoscopic Hydrodilatation • Intravenous general anesthesia or spinal anesthesia • Inserting cystoscopy lightly, do not evacuate bladder completely • Inspection the whole bladder for vasculature and lesions • The fluid level is set at 80 cm water above symphysis pubis • Fully distended the bladder • Evacuation of the bladder slowly and observe any glomerulation, petechial, splotch hemorrhage or mucosal laceration • Refilled the bladder and check ulceration • Take bladder biopsy if necessary
Interstitial cystitis in Men • Less than 10% of IC are men • 35/60 (58%) men with non-bacterial prostatitis or prostatodynia had petechiae following cystoscopic dilation • In 29 men with IC, misdiagnosis wasmade as prostatitis (48%), BPH (38%) • Carcinoma in situ should be ruled out
Management after cystoscopic Hydrodilatation for IC • Indwelling a Foley catheter especially after bladder biopsy • Adequate hydration • Hemorrhage is usually not a problem • Analgesics for severe irritative symptoms • Remove the catheter after fully awakened
Basic urodynamic abnormalities • Sensory urgency • Intolerance to increments of bladder volume • Decrease in bladder compliance <30ml/cm water (16/30 v 3/17 PBS, p<0.025) • Smaller maximal capacity under anesthesia (548 v 612, p<0.05)
Urodynamic findings in IC • 50 patients with painful bladder underwent urdynamic study and cystoscopic hydrodilation • 30 (28 F & 2 M) had characteristic IC, 20 non-IC • Symptomatology was indifferent between IC & non-IC
Uroflowmetry in IC • Most IC patients present with abnormal flow pattern • With or without a low maximal flow rate (22/28), but this feature also can be found in non-IC (11/16) • Can rule out other hypersensitive bladder and bladder outlet obstruction
Urodynamic parameters in IC • Bladder hypersensitivity FSF <100ml • A trend toward smaller capacity in chronic cases • Most have normal compliance in early IC and decreased compliance in classic IC • Most have a normal flow rate • Urethral pressure profile has no clinical value • As prognostic indicators and surgical results
Microscopic findings in IC • Classical IC – mucosal ulceration with granulation tissue; marked mononuclear cell infiltration; increased mast cell in lamina propria and detrusor; presence of intraurothelial mast cell; perineural inflammatory cell; significant fibrosis • Early IC – mucosal rupture; suburothelial hemorrhage; scanty inflammation and mild submucosal edema
Physiology of Micturition • Bladder sensation: first sensation 150ml, full sensation 250-350ml, urge sensation 400-500ml • Sensory afferents – reflex center S2-4 – micturition center (pons) – cerebral cortex • Voiding pressure in women 20-40 cm water, men 30-50 cm water
Vesical Blood Urine barrier • Urothelium appears to be a functional extension of renal collecting duct • Absence of barrier allows recirculation of renal waste and deteriorate function • 13:1 mucosal to muscular blood flow in bladder wall ratio imply a barrier function for blood-urine compound exchange and equilibrium
Increased bladder mucosal permeability • Acute bacterial cystitis • Chronic cystitis • Foreign body, calculi, tumor • Overdistension • Acidic fluid or toxin substance • Surgical trauma or instrumentation
Increased permeability of Bladder epithelium • Bladder capacity was decreased by K, hyperosmolar, and PH5; while increased by hypoosmolarity electrolyte free media, furosemide, and PH8 • Normal subjects absorbed 4.3%, IC 25% of concentrated urea from bladder • Frequent voiding reduced urinary contact time, protecting from urine recirculation
Pathophysiology of Leaky epithelium and cystometry • Impairment of blood urine barrier led to a decrease in compliance and capacity • Isotonic KCl and hyperosmolar NaCl induced an immediate onset of voiding contraction in rat bladders • CMG in normal bladder revealed no such effects of KCl & hyperosmolar NaCl • Urge sensation and pressure are elicited in diseased human bladder after intravesical K
Potassium and Bladder control • Bladder sensory afferent pathway relative to submucosal K and intramuscular proprioceptor to to intravesical pressure and tension • Intravesical K or hyperosmolarity affects exteroception resulting in reflective storage pressure elevation and urge proprioception • Local or perimuscular K enhancement facilitates onset of voiding contraction
Glycosaminoglycan & Frequency urgency syndrome • A subset of frequency urgency syndrome has a leaky epithelium and cations (K) can diffuse subepithelially and provoke urgency frequency • Intravesical KCl (0.4M) provoked symptoms in 4.5% normal, 70%IC, 18% heparin treated IC, 100% irradiation cystitis • Intravesical sulfated polysaccharide can restore injured urothelium to normal
Pathophysiology of Leaky Epithelium • Hyperosmolar NaCl concentration decreased more rapidly in over-distension, retention, bacterial and chronic cystitis • Serious water inflow and recirculation of renal waste occurred in urine retention • In experimental cystitis, slow blood flow rate resulted in maximal hyperosmolar suburothelial urea accumulation (maximal exchange)
Treatment of Interstitial Cystitis • Cystoscopic hydrodilatation • Intravesical heparin therapy • Intravesical DMSO instillation • Intravesical capsaicin or resiniferatoxin • Sodium pentosan polysulfate (PPS, Elmiron) • Amitriptynin • Supratrigonal cystectomy augmentation
Medical treatment of IC • Cyclosporine • Methotrexate • Tice strain BCG– 60% response rate vs 27% in placebo • Elmiron (PPS 100mg tid) – 6.2% to 18.7% response rate • Electromotive administration of intravesical lidocaine & dexamethasone – 62% effective
Inravesical Heparin therapy • Patients with urgency frequency and a positive potassium test • Intravesical Heparin 25000u/10ml saline and holding for 2 hours • 2x or 3x per week for 12 weeks • 67% patients have improvement in symptoms and increase in bladder capacity
The changes of urodynamic parameters before and after heparin treatment
Intravesical Capsaicin Therapy • Capsaicin in 10 uM concentration instilled intravesically 1/week to 10 women with hypersensitive bladder(HSB) and 10 with interstitial cystitis, a total 6 weeks • 8 HSB responded for 3-5 days, 2 IC responded for 2-3 days • No reported side effects
Cystoscopic hydrodilatation • Under general or spinal anesthesia, at pressure of 80cm water, the bladder was distended for 30min • Effective in relieving symptoms after hydrodilatation • The increased bladder capacity was limited • Regular hydrodilatation is needed