Download
1 / 34
400 likes | 697 Views
Risk Assessment and Risk Reduction in Women with non Hereditary BC Risk. Fabienne Liebens MD Breast Unit Isala Breast Cancer Prevention Center CHU Saint Pierre – ULB-VUB Brussels. Breast Cancer Prevention WHO definitions. Primary prevention : covers all activities designed

E N D
Risk Assessment and Risk Reduction in Women with non Hereditary BC Risk Fabienne Liebens MD Breast Unit Isala Breast Cancer Prevention Center CHU Saint Pierre – ULB-VUB Brussels
Breast Cancer PreventionWHO definitions • Primary prevention: covers all activities designed • to reduce the incidence of an illness in a population • to reduce the risk of new cases appearing • Secondary prevention:(early screening/diagnosis) • to reduce the prevalence of an illness in a population • to reduce its duration • Tertiary prevention: • to reduce the incidence of chronic incapacity or recurrences in a population, • to reduce the functional consequences of an illness • knowledge of independent risk factors of the disease • efficient risk reduction options FL - BBM2 - 2008
Risk Assessment and Risk Reduction • Why do we need to address these issues? • Are there effective preventive strategies? • How do we assess BC risk? • How could we refine risk and predict benefit of interventions? • Challenges/Conclusion? FL - BBM2 - 2008
Risk Assessment and Risk Reduction • Why do we need to address these issues? • Are there effective preventive strategies? • How do we assess BC risk? • How could we refine risk and predict benefit of interventions? • Challenges/Conclusion? FL - BBM2 - 2008
Breast Cancer Risk AssessmentWhy ? Burden of BC European BC • 2006 • 430 000 cases • 132 000 deaths • Life time risk approaching 1 in 9 women • Demographic increase • Ageing population • Rise in young women • Wide differences in survival (16%) Eurocare 3 Adapted from Dr Nick Perry, Europa Donna Pan-European Conference- Amsterdam 2007 FL - BBM2 - 2008
Belgian Cancer Patients’ Needs StudyFrequency of difficulties encountered Assessment of 38 types of difficulties (psychosocial, physical, marital, sexual…) More than 26 difficulties 6,3% From 21 to 25 difficulties 14,0% From 16 to 20 difficulties 28,7% From 11 to 15 difficulties 23,7% From 6 to 10 difficulties 17,9% From 1 to 5 difficulties 9,4% No difficulty 0 % % FL - BBM2 - 2008 2005- Courtesy of Darius Razavi and Isabelle Merckaert
Breast Cancer Risk AssessmentWhy ? Risk Factors Breast Density 5-10% >25% Tamoxifen FL - BBM2 - 2008
Risk Assessment and Risk Reduction • Why do we need to address these issues? • Are there effective prevention strategies? • How do we assess BC risk? • How could we refine risk and predict benefit of interventions? • Conclusion? FL - BBM2 - 2008
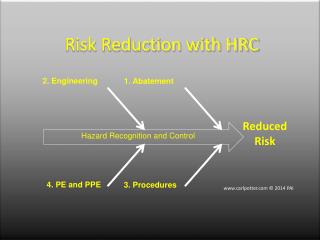
Prevention strategies Adapted from Ozane EM. The Breast Journal 2006; 12: 103-133. FL - BBM2 - 2008
Breast Cancer Risk AssessmentWhy ? Preventive strategies • Tamoxifen/raloxifen • Prophylactic surgery • Life style modifications the net risk/benefit ratio depends on the ability to quantify accurately a woman’s baseline likelihood of developing breast cancer Bishop J et al. The Health Economic of chemoprevention for Breast Cancer in Australia. Cancer Institute NSW, June 2008 FL - BBM2 - 2008
Risk Assessment and Risk Reduction • Why do we need to address these issues? • Are there effective prevention strategies? • How do we assess BC risk? • How could we refine risk and predict benefit of interventions? • Conclusion? FL - BBM2 - 2008
How do we assess BC risk? Models Gail, Claus, Tyrer Cuzick • The most common models used to predict a woman’s risk of breast cancer BRCAPRO, Frank, Cough • Used in a subset of the high-risk population to predict a woman’s probability of having a genetic mutation FL - BBM2 - 2008
Breast Cancer Risk AssessmentHow ? Models • The Gail risk assessment model • estimates the risk of developing breast cancer in women undergoing annual screening. • Gail et al used data from 284,780 predominately white women in 28 participating centers of the Breast Cancer Detection Demonstration Project (BCDDP) to develop the model. • An unconditional logistic regression model • based on the ratio of risk in a woman with specified risk factors compared with the risk in a woman with no risk factors. FL - BBM2 - 2008
YES 51 NO 1 12 0 0 1 FL - BBM2 - 2008
Breast Cancer Risk AssessmentHow ? Models: Gail Limitations • Does not show great discriminatory power (predicts population risk well, but not individual risk). • 58%-65%-73% discriminatory • Not sufficient family history • Rockhill et al. J Natl Cancer Inst 93:358, 2001. • Tice. Breast Ca Res Treat 88(suppl 1):2004; abstract 13 • Cuzick. ASCO Educational Session 2005. Advantages • Use is widespread, with many forms of access (National Cancer Institute [NCI] Web site, handheld and computer applications). • Applicable to the largest number of women • Has been validated • Has been shown to be well calibrated. FL - BBM2 - 2008
Breast Cancer Risk AssessmentHow ? Models Conclusion: It is not sufficient to use only these mathematical models for the purpose of individual decision making regarding prevention interventions. FL - BBM2 - 2008
Risk Assessment and Risk Reduction • Why do we need to address these issues? • Are there effective prevention strategies? • How do we assess BC risk? • How could we refine risk and predict benefit of interventions? • Conclusion? FL - BBM2 - 2008
Breast Cancer Risk AssessmentOptions to Refine Risk and Predict Benefit of Intervention • - To improve individualized risk assessments • - To tailor prevention care Biomarkers Breast Density Histologic or Cytologic evidence of atypia FL - BBM2 - 2008
Mammographic DensityOptions to Refine Risk and Predict Benefit of Intervention • Reflective of amount of epithelium, stroma, and fluid relative to fat. • Stroma and collagen make up the bulk of density. • Strong hereditary component Risk biomarker for both ER + and ER - cancers in pre- and postmenopausal women. Boyd et al. Lancet Oncol 2005 6(10):798-808. McCormack VA et al. Cancer Epidemiol Biomarkers Prev. 2006 5(6):1159-69. Chen J. et al. J Natl Cancer Inst 2006; 98: 1215-1226. FL - BBM2 - 2008
Risk of Breast Cancer According to Breast Density in Premenopausal and Postmenopausal Women RR=5.3 RR=3.4 FL - BBM2 - 2008 Santen et al. N Engl J Med 2005;353:275
Agreement between computer-assisted quantitative measurement of mammographic breast density (MBD) and clinicians' assessment. F. Liebens et al. Proceedings of EBCC-6; European Journal of Cancer 2008; 6 (7):63. (abstract 45). FL - BBM2 - 2008
Breast Cancer Risk AssessmentOptions to Refine Risk and Predict Benefit of Intervention • - To improve individualized risk assessments • - To tailor prevention care Biomarkers Breast Density Histologic or Cytologic evidence of atypia FL - BBM2 - 2008
Proliferative benign breast disease with atypia 19/100 15y Degnim AC et al. JCO 2007 25:2671-2677 Elmore, J. G. et al. N Engl J Med 2005;353:297-299 FL - BBM2 - 2008
Multifocal occult hyperplasia (+/- Atypia) is prevalent in young and middle aged high risk women But 80% of women have never had a diagnostic biopsy Hoogerbrugge et al. JCO 2003 21:41 Schnitt. Amer J Surg Pathology 2003 27:836 FL - BBM2 - 2008
New methods Nipple aspiration fluid NAF Ductal Lavage DL Random peri areolar fine-needle aspiration RPFNA • RPFNA • Efficient way to obtain tissue for a prevention trial(Fabian et al Frontiers Prev Res 2005) • Cost effective to determine who gets chemoprevention (Ozanne et al Cancer Epidemiol Bio Prev 2004) • Women with AH more likely to enroll on NSABP Prevention Trial (Vogel et al JNCI 2002) and to take tamoxifen(Goldenberg VK Cancer Epidemiol Bio Prev 2007) cytology Risk Prediction FL - BBM2 - 2008
Cytologic findings Adapted from Arun, B. et al. Clin Cancer Res 2007;13:4943-4948 FL - BBM2 - 2008
Models for Phase II Chemoprevention Trials for Women at High Risk of BC Tissue Based Biomarkers R A N D O M I Z A T I O N Morphology Proliferation Study Agent RPFNA Random periareolar fine needle aspiration Repeat Biomarkers 6-12 months DL Ductal lavage NAF Nipple aspiration fluid Placebo Imaging-Based Biomarkers Mammographic Breast density Adapted from Fabian C. Endocrine related Cancer 2005 FL - BBM2 - 2008
Breast Cancer Risk AssessmentWhy and How ? Clinical Practice • AIM of a consultation about breast cancer risk assessment • to determine if risk level is high enough to warrant special surveillance measures or prevention interventions, • if so, motivate those at high risk to partake in surveillance/prevention options • reassure those at low/moderate risk NCNN Breast Cancer risk reduction V2.2007 Kushi LH. CA Cancer J Clinic 2006 Sivell S. Cochrane databases of systematic reviews 2007 Kiluk J. Cancer Control 2007 FL - BBM2 - 2008
FL - BBM2 - 2008 European Journal of Cancer Prevention 2008 in press
Breast Cancer Risk AssessmentChallenges • Improve woman’s awareness/Knowledge? • Best practice in risk communication ? • Cost effectiveness ? • Best biomarker that predicts both risks and benefits fromintervention ? • Improve the skills of primary care providers ? FL - BBM2 - 2008
“…Cancer is a multistage disease, not a single event, and doctors should emphasize cancer prevention in addition to cancer treatment and cure…” Peter Greenwald, Division of Cancer Prevention, National Cancer Institute. FL - BBM2 - 2008
“…Life is a sexually transmitted disease and there is a 100% mortality rate. …” Woody Allen FL - BBM2 - 2008