Download
1 / 1
10 likes | 181 Views
Implementing Addiction Treatment Trials in Medical Settings in (NIDA’s) National Drug Abuse Treatment Clinical Trials Network A.A. Forcehimes 1 , M.P. Bogenschutz. 1 , D.M. Donovan 2 , C. Crandall 1 , R. Lindblad 3 , R. Mandler 4 , H.I Perl 4 , R. Walker 5

E N D
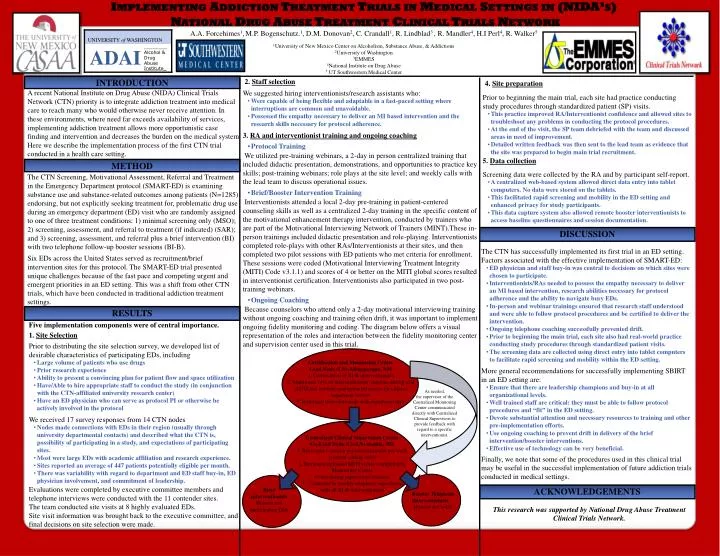
Implementing Addiction Treatment Trials in Medical Settings in (NIDA’s) National Drug Abuse Treatment Clinical Trials Network A.A. Forcehimes1,M.P. Bogenschutz.1, D.M. Donovan2, C. Crandall1, R. Lindblad3 , R. Mandler4, H.I Perl4, R. Walker5 1University of New Mexico Center on Alcoholism, Substance Abuse, & Addictions 2University of Washington 3EMMES 4National Institute on Drug Abuse 5 UT Southwestern Medical Center INTRODUCTION • 2. Staff selection • We suggested hiring interventionists/research assistants who: • Were capable of being flexible and adaptable in a fast-paced setting where interruptions are common and unavoidable. • Possessed the empathy necessary to deliver an MI based intervention and the research skills necessary for protocol adherence. • 3. RA and interventionist training and ongoing coaching • Protocol Training • We utilized pre-training webinars, a 2-day in person centralized training that included didactic presentation, demonstrations, and opportunities to practice key skills; post-training webinars; role plays at the site level; and weekly calls with the lead team to discuss operational issues. • Brief/Booster Intervention Training • Interventionists attended a local 2-day pre-training in patient-centered counseling skills as well as a centralized 2-day training in the specific content of the motivational enhancement therapy intervention, conducted by trainers who are part of the Motivational Interviewing Network of Trainers (MINT).These in-person trainings included didactic presentation and role-playing. Interventionists completed role-plays with other RAs/Interventionists at their sites, and then completed two pilot sessions with ED patients who met criteria for enrollment. These sessions were coded (Motivational Interviewing Treatment Integrity (MITI) Code v3.1.1) and scores of 4 or better on the MITI global scores resulted in interventionist certification. Interventionists also participated in two post-training webinars. • Ongoing Coaching • Because counselors who attend only a 2-day motivational interviewing training without ongoing coaching and training often drift, it was important to implement ongoing fidelity monitoring and coding. The diagram below offers a visual representation of the roles and interaction between the fidelity monitoring center and supervision center used in this trial. • 4. Site preparation • Prior to beginning the main trial, each site had practice conducting study procedures through standardized patient (SP) visits. • This practice improved RA/Interventionist confidence and allowed sites to troubleshoot any problems in conducting the protocol procedures. • At the end of the visit, the SP team debriefed with the team and discussed areas in need of improvement. • Detailed written feedback was then sent to the lead team as evidence that the site was prepared to begin main trial recruitment. • 5. Data collection • Screening data were collected by the RA and by participant self-report. • A centralized web-based system allowed direct data entry into tablet computers. No data were stored on the tablets. • This facilitated rapid screening and mobility in the ED setting and enhanced privacy for study participants. • This data capture system also allowed remote booster interventionists to access baseline questionnaires and session documentation. A recent National Institute on Drug Abuse (NIDA) Clinical Trials Network (CTN) priority is to integrate addiction treatment into medical care to reach many who would otherwise never receive attention. In these environments, where need far exceeds availability of services, implementing addiction treatment allows more opportunistic case finding and intervention and decreases the burden on the medical system Here we describe the implementation process of the first CTN trial conducted in a health care setting. METHOD The CTN Screening, Motivational Assessment, Referral and Treatment in the Emergency Department protocol (SMART-ED) is examining substance use and substance-related outcomes among patients (N=1285) endorsing, but not explicitly seeking treatment for, problematic drug use during an emergency department (ED) visit who are randomly assigned to one of three treatment conditions: 1) minimal screening only (MSO); 2) screening, assessment, and referral to treatment (if indicated) (SAR); and 3) screening, assessment, and referral plus a brief intervention (BI) with two telephone follow-up booster sessions (BI-B). Six EDs across the United States served as recruitment/brief intervention sites for this protocol. The SMART-ED trial presented unique challenges because of the fast pace and competing urgent and emergent priorities in an ED setting. This was a shift from other CTN trials, which have been conducted in traditional addiction treatment settings. DISCUSSION • The CTN has successfully implemented its first trial in an ED setting. Factors associated with the effective implementation of SMART-ED: • ED physician and staff buy-in was central to decisions on which sites were chosen to participate. • Interventionists/RAs needed to possess the empathy necessary to deliver an MI based intervention, research abilities necessary for protocol adherence and the ability to navigate busy EDs. • In-person and webinar trainings ensured that research staff understood and were able to follow protocol procedures and be certified to deliver the intervention. • Ongoing telephone coaching successfully prevented drift. • Prior to beginning the main trial, each site also had real-world practice conducting study procedures through standardized patient visits. • The screening data are collected using direct entry into tablet computers to facilitate rapid screening and mobility within the ED setting. • More general recommendations for successfully implementing SBIRT in an ED setting are: • Ensure that there are leadership champions and buy-in at all organizational levels. • Well trained staff are critical: they must be able to follow protocol procedures and “fit” in the ED setting. • Devote substantial attention and necessary resources to training and other pre-implementation efforts. • Use ongoing coaching to prevent drift in delivery of the brief intervention/booster interventions. • Effective use of technology can be very beneficial. • Finally, we note that some of the procedures used in this clinical trial may be useful in the successful implementation of future addiction trials conducted in medical settings. RESULTS • Five implementation components were of central importance. • 1. Site Selection • Prior to distributing the site selection survey, we developed list of desirable characteristics of participating EDs, including • Large volume of patients who use drugs • Prior research experience • Ability to present a convincing plan for patient flow and space utilization • Have/Able to hire appropriate staff to conduct the study (in conjunction with the CTN-affiliated university research center) • Have an ED physician who can serve as protocol PI or otherwise be • actively involved in the protocol • We received 17 survey responses from 14 CTN nodes • Nodes made connections with EDs in their region (usually through university departmental contacts) and described what the CTN is, possibility of participating in a study, and expectations of participating sites. • Most were large EDs with academic affiliation and research experience. • Sites reported an average of 447 patients potentially eligible per month. • There was variability with regard to department and ED staff buy-in, ED physician involvement, and commitment of leadership. • Evaluations were completed by executive committee members and telephone interviews were conducted with the 11 contender sites. • The team conducted site visits at 8 highly evaluated EDs. • Site visit information was brought back to the executive committee, and final decisions on site selection were made. Certification and Monitoring Center Lead Node (LN)-Albuquerque, NM 1. Certification of BI-B interventionists 2. Monitored 14% of interventionists’ sessions during trial (MITI and content) and uploaded scores for clinical supervisor review 3. Red-lined interventionists with significant drift As needed, the supervisor of the Centralized Monitoring Center communicated directly with Centralized Clinical Supervisors to provide feedback with regard to a specific interventionist. Centralized Clinical Supervision Center Co-Lead Node (Co-LN)-Seattle, WA 1. Reviewed 1 session per interventionist per week (content coding only) 2. Reviewed uploaded MITI scores completed by Monitoring Center to use during supervision sessions 3. Conducted bi-weekly telephone supervision with all BI-B interventionists ACKNOWLEDGEMENTS Brief Interventionists Housed at 6 participating EDs Booster Telephone Interventionists Housed at Co-LN This research was supported by National Drug Abuse Treatment Clinical Trials Network.