Download
1 / 29
290 likes | 697 Views
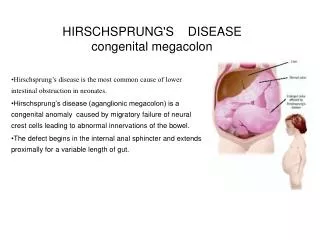
Hirschsprung’s Disease: Options for Surgical Correction. George W. Holcomb, III, M.D., MBA Children’s Mercy Hospital Kansas City, Missouri. Hirschsprung’s Disease. Principles Barium enema for suspected disease Anorectal biopsy for confirmation of diagnosis

E N D
Hirschsprung’s Disease: Options for Surgical Correction George W. Holcomb, III, M.D., MBA Children’s Mercy Hospital Kansas City, Missouri
Hirschsprung’s Disease Principles • Barium enema for suspected disease • Anorectal biopsy for confirmation of diagnosis • Selection of operation based on extent of disease – need biopsy of ganglionated colon
Hirschsprung’s Disease Historical Approach • Colostomy at diagnosis • Pullthrough 6 - 12 months later • Duhamel • Soave • Swenson
Hirschsprung’s DiseaseCurrent Surgical Options One-stage Swenson Duhamel Soave Laparoscopic-assisted Transanal Two-stage Swenson Duhamel Soave (Laparoscopic-assisted) (Transanal)
Hirschsprung’s Disease • One stage operation for rectosigmoid disease is current preferred approach • Laparoscopic-assisted or transanal approach best suited for typical rectosigmoid disease • Unclear (in my mind) whether one or two stage procedure is best for disease proximal to splenic flexure
Hirschsprung’s Disease • Initial trans-abdominal biopsy with frozen section is important in determining what surgical option is best for each patient • Biopsy can be performed through umbilicus easily
Hirschsprung’s Disease Extent of DiseaseOptimal Surgical Option Rectosigmoid Laparoscopic-assisted or transanal Descending colon Laparoscopic-assisted Transverse colon Two-stage approach Rt colon; ileum Two-stage approach Ileal pullthrough (? Laparoscopic)
Hirschsprung’s Disease Personal Approach • Laparoscopic directed biopsy thru umbilicus • For rectosigmoid disease, laparoscopic assisted pullthrough • Tension free relocation of ganglionic colon to anus • Already in abdomen for laparoscopic directed biopsy
Patient Positioning • Baby across O.R. table • Circumferential, full body prep • Urinary catheter
Port Positioning • Port placement • 5 mm umbilical • 5 mm RUQ • 5 mm RLQ • 3 mm (optional) LUQ
Technique Ligation of mesenteric vessels
Technique Mobilization of rectum
Technique Mobilization of rectum
Technique Mobilization of left colon
Laparoscopic Pullthrough • Laparoscopic mobilization of recto-sigmoid vasculature • Extracorporeal endorectral dissection
Technique Completed pullthrough
Laparoscopic Pullthrough Primary Procedure - No Colostomy
Transanal Approach • Best suited for low rectosigmoid disease • Concern is tension on vasculature as it is brought to anus • Appropriate technique if transabdominal biopsy is performed to define extent of disease • If biopsy done, why not mobilize laparoscopically? • If no biopsy, must be ready to do transverse colon or ileal pullthrough in newborn period
Hirschsprung’s DiseasePrimary Pullthrough • Obviates need for colostomy care • Second operation and hospitalization not required • Normal bowel function established early • Reduced cost of care
Mean # PtsAge (Wk)Wt(kg) 7 36 6.41 (1 - 138) (2.7 - 11.5) 8 27 7.24 (12 - 54) (5.3 - 8.1) Children’s Mercy HospitalResults2000 - 200115 Pts Primary Lap Pullthrough Colostomy + Open Pullthrough
Total Postop Total Hospitalization(D) Cost ($) 3.7 $38,489 (3-7) (21,040 - 71,034) 3.4 + 3.5 $70,858 (2-19) (2-4) (20,087 - 165,642) Children’s Mercy HospitalResults Primary Lap Pullthrough Colostomy + Open Pullthrough
Open + transanal 1990’s Allows biopsy Good results Laparoscopy + transanal Allows biopsy Mobilization of rectum, sigmoid, left colon Good early results Hirschsprung’s DiseasePrimary Pullthrough • Transanal approach alone • No ABD exploration • Pt. selection very important • Good early results
Postoperative Care • Biggest problem is enterocolitis
Postoperative Management • Anorectal dilations • Begin 3rd week, Hegar 8 BID • Advance to Hegar 14 QD, then QOD, then Q3D, up to Q week • Flagyl/anorectal irrigations if develop enterocolitis • Personal Experience (50 cases/7 yrs) • All well except 2 with colostomy (one closed)
Summary • Functional results following pullthrough are probably similar b/w approaches • Patient selection important for primary pullthrough regardless of approach • Laparoscopic one stage approach affords good results, has less total hospitalization and is less costly than two stage approach