Download
1 / 25
260 likes | 412 Views
Managing Key but Disruptive Professionals. Michael J. Herkov , Ph.D., ABPP P. O . W. E. R. University of Florida A program of Life Enhancement Skills for Disruptive Professionals. Disruptive Behavior (DB) is Not. Constructive criticism Expression of dissatisfaction

E N D
Managing Key but Disruptive Professionals Michael J. Herkov, Ph.D., ABPP P.O.W.E.R.University of Florida A program of Life Enhancement Skills for Disruptive Professionals
Disruptive Behavior (DB) is Not • Constructive criticism • Expression of dissatisfaction • Regular grievance process • Legitimate use of litigation process
Definition of DB • No OSHA definition of bullying • Verbal or physical • Harassing behavior • Against a protected class • e.g., race, religion, gender, etc. • Washington Dept. of Labor and Industries • Any incident in which a person is abused, threatened or assaulted including harassment, bullying, intimidation, physical threats… and other intrusive behaviors
AMA Definition of DB • Profane, disrespectful or belittling language • Personal sarcasm or cynicism • Deliberate lack of cooperation • Physical intimidation, contact or threat • Throwing objects • Repeated threats of litigation • Any behavior that harms or intimidates others so that quality is compromised
DB in Medicine Rosenstein & O’Daniel (2008) Jt Comm J Qual Patient Saf. 34; 464-71 • Statistics • 97% of physicians and nurses experienced DB at work • 77% witnessed physician disruption • 65% witnessed nurse disruption • 40% were intimidated into silence about questionable practice by a disruptive physician • 3%-5% of physicians display DB
Consequences of DB in Medicine • Rosenstein & O’Daniel Study (2008) • 67% reported link with adverse events • 71% reported link to medication errors • 27% reported link to patient mortality • 18% were aware of an adverse event linked to DB • 64% of pharmacists assumed an order was correct, rather than interact with a DP
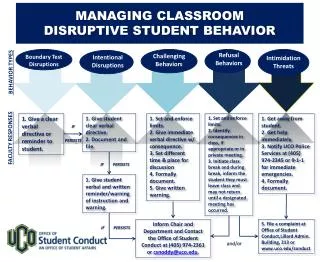
Medicine Response to DB • The Joint Commission (TJC) required hospitals to develop: • A code of conduct that defines DB • A process for managing DB • Codes that incorporate interpersonal skills and professionalism to the credentialing process
Staff Consequences of DB • Victims of DB report: • Physical symptoms • Low morale • Depression • Anger • Dysfunction at home • 68% considered leaving their job • 41% transferred or left the position • $60,000 to replace a skilled nurse
Reasons for Not Reporting DB Colleen.thornburgh@studergroup.com 35% did not believe it would have a positive outcome 46% believe administration not committed to addressing DB 60% believe DB is ignored in “high value” professionals 18% fear reprisal or career jeopardy
DB in Business WBI US Workplace Bullying Survey 2010 • Zogby 2010 • 4,210 respondents • DB definition • Abusive conduct by superiors and co-workers manifested by: • sabotage • verbal abuse • threatening conduct • intimidation • humiliation
WBI Results • Most bullying is legal • 4 times more common than sexual harassment • Gender of bullies • 62% men • 38% women • Organization • Equal rates in small to large organizations and public and private sectors
Specific Bullying Behavior Salin, D. (2001). European J of Work and Educational Psychology, 10, 4, 425-441
Personal Consequences Privitera & Campbell (2009) Cyberbullying: the new face of workplace bullying? CyberPsychology & Behavior, 12, 4, 395-400. Decreased immune system and increased illness Reduced self-esteem Increased depression Increased family problems Decreased job satisfaction Reduced job commitment
Organizational Consequences Increased absenteeism Decreased morale Reduced efficiency and productivity Breakdown of work relationships and teams Increased staff turnover Litigation costs Decreased profitability
New York legislation allows civil suit for workers physically, psychologically or economically abused on the job Employers responsible for the bullying by supervisors and colleagues Legal Issues www.healthyworkplacebill.org
Etiology of DB CHANGING BEHAVIOR STANDARDS LACK OF ASSERTIVENESS SKILLS CULTURE OF ABUSE DISRUPTIVE BEHAVIOR POOR COMMUNICATION SKILLS POOR STRESS MANAGEMENT SUBSTANCE ABUSE AXIS I MENTAL ILLNESS AXIS II MENTAL ILLNESS
HR Policy Suggestions • Education of all staff on appropriate behavior • Didactic instruction similar to diversity and sexual harassment training • Post-test assessment • Mandatory compliance
HR Policy Suggestions • Policies for evaluating and correcting DB • Inclusion in employee handbook • Part of contracts and collective bargaining • Holding all staff equally accountable • Clear action plan in DB for: • making complaints • investigating complaints • deciding complaints
HR Policy Suggestions • Evaluation Process • External versus internal evaluation • Objective • Specialized and Expert • Confidential • Treatment recommendations • Monitoring and follow-up
Treatment Philosophy Most people “do the best they can with what they’ve got.” State not trait-based behavior Everyone can improve her interaction skills. Change is not about masking undesirable behaviors in the workplace, but learning a new, better WAY TO BE.
Evaluation Process • 2-day Assessment • Clinical interview • Psychological testing • Collateral data interviews • Feedback session with professional and referring agency • Treatment recommendations
Program Options • Outpatient Treatment • Individual therapy • Seminar/Workshop • 3-4 days • Didactic instruction • Residential Program • Didactic and experiential training • Therapeutic community
Program Components • Didactic and Experiential Treatment • Self-discovery • Communication skills • Anger management • Stress management • Physical wellness • Spiritual development • Individual therapy
Aftercare Components • Treatment Planning • Anticipation and addressing of R-T-W issues • Support group follow-up • Monitoring
Questions or Comments Thank you for participating in today’s webinar!