Download
1 / 21
300 likes | 624 Views
The Global Epidemiology and Challenge of Osteoporosis. Ethel S. Siris, MD Madeline C. Stabile Professor of Clinical Medicine Director, Toni Stabile Osteoporosis Center Columbia University Medical Center New York, NY. Pathogenesis of Osteoporotic Fractures. Sporadic Factors.

E N D
The Global Epidemiology and Challenge of Osteoporosis Ethel S. Siris, MD Madeline C. Stabile Professor of Clinical Medicine Director, Toni Stabile Osteoporosis Center Columbia University Medical Center New York, NY
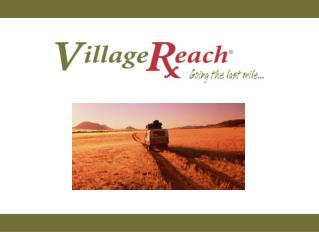
Pathogenesis of Osteoporotic Fractures Sporadic Factors Reduced Bone Quantity (and Quality) Heredity Low Peak Bone Mass Local Factors FRACTURES Increased Bone Loss Menopause Falls Aging
Prevalence of Osteoporosis • Affects 200 million women worldwide1 • 1/3 of women aged 60 to 70 • 2/3 of women aged 80 or older • Approximately 30% of women over the age of 50 have one or more vertebral fractures2 • Approximately one in five men over the age of 50 will have an osteoporosis-related fracture in their remaining lifetime1 1. IOF, 2005 (www.osteofound.org) 2. Dennison E and Cooper C. Horm Res. 2000;54 suppl 1:58-63.
US Report: Osteoporosis is Under Diagnosed and Under Treated • Osteoporosis affects approximately 8 million women and 2 million men in the United States; 34 million more have low bone mass1 • A diagnosis of osteoporosis or vertebral fracture is made by <2% of primary care physicians2 • Drug therapy is offered to only 36% of diagnosed patients • National Osteoporosis Foundation. At: http://www.nof.org/advocacy/prevalence. Accessed August 2005; • 2. Gehlbach et al. Am J Public Health. 2002;92:271.
US Report: Bone Density Testing • Currently, only 20% of patients for whom bone density testing by DXA is indicated by the USPSTF recommendations (women 65 and older, women 60-64 with risk factors) undergo this critical test for diagnosis and risk of future fracture. • Coverage of BMD testing is limited in older men – e.g. not covered by Medicare after hip fracture in men. • Planned reductions by Medicare in the reimbursement for BMD testing threaten to reduce the number of facilities available to patients, which may further limit access to DXA.
Remaining lifetime fracture risk (%) in Caucasian population at the age of 50 Type of FractureMen Women Forearm 4.6 20.8 Hip 10.7 22.9 Spine 8.3 15.1 Proximal humerus 4.1 12.9 Any 22.4 46.4 Kanis JA et al. Osteoporos Int. 2000:11:669-674.
Morbidity After Vertebral Fractures • Back pain • Loss of height • Deformity (kyphosis, protuberant abdomen) • Reduced pulmonary function • Diminished quality of life: loss of self-esteem, distorted body image, dependence on narcotic analgesics, sleep disorder, depression, loss of independence
Hip fractures are associated with increased morbidity and mortality Unable to carry out at least one independent activity of daily living 80% One year after an hip fracture: Unable to walk independently Patients (%) 40% Permanent disability Death within one year 30% 20% Cooper C. Am J Med. 1997;103(2A):12S-17S.
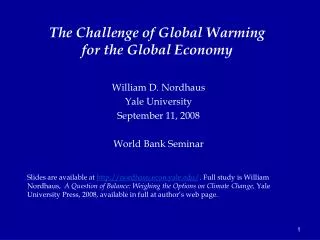
Survival after hip fracture Expected survival in the general population 1.00 0.75 Women Men Survival probability 0.50 Hip fractured Women 0.25 Hip fractured Men 0.00 0 10 2 4 6 8 Time after hip fracture (years) Trombetti A et al. Osteoporos Int. 2002;13:731-737.
Costs Associated with Osteoporotic Fractures in the USA 20 • Direct costs for osteoporotic fractures range from $12.2 to $17.9 billion, measured in 2002 dollars. 18 16 14 12 10 2002 Dollars, billion • Indirect costs (including lost productivity for the patient and for family members who must provide care for the patient) could add billions. 8 6 4 2 0 US Department of Health and Human Services. Available at: www.surgeongeneral.gov/library/bonehealth/docs/exec_summ.pdf. Accessed August 24, 2005.
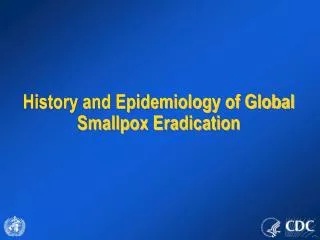
1950 1950 2050 2050 Projected Number of Hip Fractures 3250 Projected to reach 3.250million in Asia by 2050 668 742 400 Total number ofhip fractures:1950 = 1.66 million 2050 = 6.26 million 378 600 629 1950 2050 100 1950 2050 Estimated no. of hip fractures: (1000s) Adapted from Cooper C et al. Osteoporosis Int. 1992;2:285-289.
Yesterday’s Failings, Today’s Opportunities • The biggest problem today is lack of awareness of bone disease by both the public and health care professionals, many of whom do not understand the magnitude of the problem or the ways in which bone diseases can be prevented and treated
It Is NOT Just About Osteoporosis… • Other congenital or acquired disorders of bone such as Paget’s disease, osteogenesis imperfecta, osteomalacia, and skeletal complications of malignancy affect a smaller but still substantial number of people in the US. • Physicians are often unaware of the clinical manifestations or means of diagnosing and treating these conditions, preventing timely introduction of appropriate management.
Everyone has a role to play in improving bone health This report is a starting point for national action
Although we should know better… • Relatively few individuals follow the recommendations related to the amounts of physical activity, calcium and vitamin D that are needed to maintain bone health • Several studies suggest that awareness of risk factors is low, and that when medical treatment is prescribed, adherence is poor, reducing the opportunity to reduce the burden of fractures
Although we should know better… • Physicians frequently fail to diagnose and treat osteoporosis, even in elderly patients who have suffered a fracture; when they do treat, they may not conform to evidence based recommendations. • A fracture is a sentinel event, and coordination between those who repair fractures and those who manage the patient to prevent the next fracture is a critical need.
FRAX™:WHO Fracture Risk Assessment Tool • Estimates the 10-year patient-specific absolute fracture risk • Hip • Major osteoporotic fracture (spine, forearm, hip, or humerus) • Developed by WHO to evaluate fracture risk of patients from epidemiologic data from the US, Europe, Australia, and Japan • Integrates clinical risk factors with femoral neck BMD, but may be performed without BMD • Incorporated into NOF treatment guidelines in the US and other country-specific recommendations • Restricted to untreated patients • It is most useful as a way to risk-stratify the patient with low bone mass (osteopenia) to aid in treatment decisions NOF = National Osteoporosis Foundation.
Although we should know better… • Managed care organizations and other insurance providers in the US for individuals under age 65 may not see the full impact of bone disease in their enrollees, since most will be enrolled in Medicare by the time they fracture; thus, they may not pay attention to bone health and to preventive strategies appropriate to the younger populations they serve
A Call to Action from the US Surgeon General • The gap between what we know and its application in the community remains large and needs to be closed • We need to focus on postmenopausal women, but must not neglect men, racial and ethnic minorities, the low income elderly, individuals with disabilities and those in rural areas
A Standard of Care • Osteoporosis risk assessment and preventive management should become a standard of care for all postmenopausal women and older men • Adequate intakes of calcium and vitamin D, exercise, and falls prevention must be emphasized • Bone density testing for diagnosis of osteoporosis and 10 year fracture probability determinations for treatment intervention offer validated tools to guide management decisions; recognition of less common bone diseases must occur • Safe and effective pharmacological therapy should be prescribed when indicated - and adherence must be achieved to maximize benefit