Download
1 / 29
290 likes | 323 Views
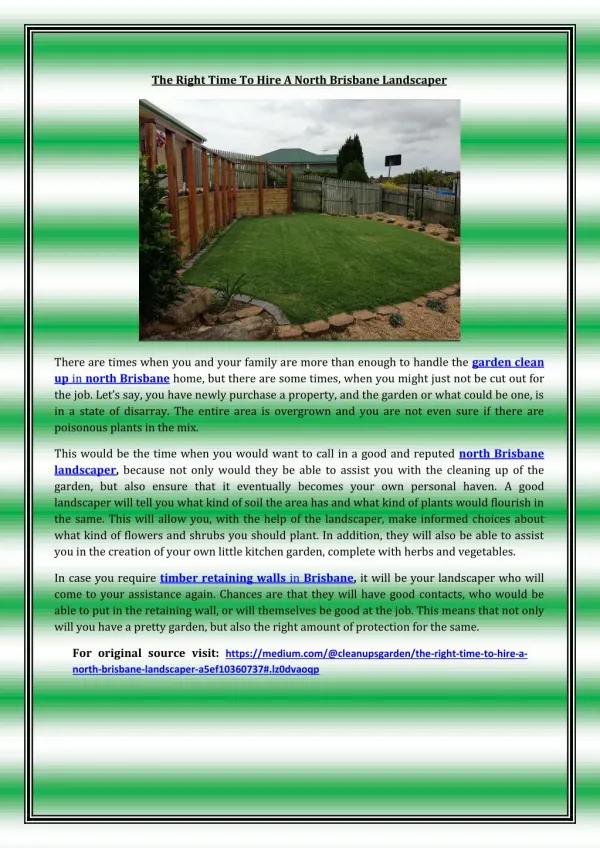
Explore systematic changes in mental health support at the North Brisbane Partners in Recovery forum. Learn about the triage system trial incorporating innovative tools and insights. Reflect on the complex interactions and interconnections influencing outcomes. Gain insights into mental illness, homelessness, and recovery principles shaping best practices. Understand the challenges and needs of clients with mental health issues and complex circumstances. Discover the framework, structures, and strategies driving systemic change. Plan for future improvements based on lessons learned and ongoing development.

E N D
Overview • About Under 1 Roof • Reflections on “systemic change” • Our framework for this project • How we went about it • What we have learned • So what and what next?
About Under 1 Roof Our members • 139 Club Inc • Bric Housing Company • Brisbane Housing Company • Brisbane Youth Service • Footprints in Brisbane • New Farm Neighbourhood Centre • Rotary Club of Fortitude Valley • Queensland Intravenous Health Network (QuIHN) • Communify Queensland • Mission Australia • Youth Emergency Services • Care Housing • Red Cross
About Under 1 Roof Our structures • Board (governance, accountability, strategy) • Quality forum (managers, focussed on implementing quality improvements) • Case coordination meetings/practice – meetings every two weeks, clients with complex needs • Learning and development: training, resources, Synthesis Series
Systemic change:Scoping of the project • To develop and trial a triage system including relevant/helpful tools which will address systemic issues and barriers to people who have a mental illness • To include a learning and development component to support change • PIR Innovation Fund: mental illness, innovation and systems focus
Systemic change:Focussing our work Not one part of something but how all of the parts add up and function together. So we had to consider: • the way the various parts of the service system relate to each other and the quality of these relationships • service delivery models and funding patterns and programs • how resources are accessed (guidelines, eligibility etc) • housing products • Information transmission, resources and infrastructure
Systemic change:Interconnections Factors impacting on outcomes Spheres of influence and change Systems are about how multiple components relate to each other and operate. Under 1 Roof, 2013
Systemic change:Tools are only part of the story • A triage system is made up of related elements • One element will be the tools that support assessment, prioritisation, case planning and plan implementation • Important that we understand a Triage System is not only a Triage Tool.
Systemic change:Requires insight • The Triage Project trial focus is on systems elements • Systems change will take thorough account of client characteristics such as mental illness. • It will have implications for practice and resources (existing and new).
Our framework: Reflecting best practice • A triage system informed by recovery principles and practices • A triage system informed by best practice in ending homelessness: • Housing first • Assertive and persistent practice • System integration • Wrap around support.
Our framework;Acknowledging complexity • Specialist homelessness services • Multi-agency involvement (beyond SHS) • Decentralised with various gateways • Social and private housing systems • People need broader resources and assistance than just a specialised homelessness response
Our framework:Understanding homelessness • Degrees of homelessness and various levels • Diverse drivers which can co-exist making the causes more complex and solutions more challenging • Diverse population groups with different needs
Our framework:Insights into mental illness • U1R: 52.2% of clients with a mental illness (2013-2014) and more with mental health issues; 70.8% presented with 2 or more complex issues; 39% with 3 or more complex issues • Homelessness is also a cause of mental ill-health – one study showed that 16% of a sample of homeless people developed mental health symptoms • SANE sample identified 90% had experienced homelessness or insecurity about their accommodation at some point • A higher proportion of Under 1 Roof clients who disengage from services live with a mental illness and/or substance use issue (61% compared to 51% for 2012-2013)
Our framework:Design for implications of mental illness… • Difficulty with medication side effects, screening out environmental stimuli: • Noise and crowds can be challenging • Sustaining concentration: restlessness, shortened attention span, distraction, and difficulty understanding or remembering verbal directions. • Maintaining stamina and difficulty sustaining an activity • Handling time pressures and multiple tasks: difficulty prioritizing tasks, and meeting deadlines. Challenges in multi-task work.
Our framework:Getting and keeping housing • Hearing and understanding information • Consideration of options and alternatives • The capacity to make plans • Receiving, interpreting and following instructions • Sequencing events and actions in the required order as part of a plan • Remembering actions that need to be taken and time frames/deadlines • Making appointments, recording times, turning up on time • Completing and submitting essential paperwork • Recounting information and progress between different services • Engaging with several important relationships (support worker, specialist help, health professionals, housing provider, private housing etc) • Travelling between appointments/inspections • Weighing up alternatives and making decisions • Arranging to move, managing belongings • Developing new, important relationships with housing option/provider, neighbours
Our framework:Access points for the homeless • Specialist homelessness services as a critical point of contact for people • Housing providers including the Housing Service Centres which are part of the Queensland Government Department of Housing and Public Works • Mental health services may also be the first point of contact for people with mental health issues and mental illness • Other specialist services in areas such as substance use • Mainstream services in the broader service system such as community centres, hospitals, police etc. • Access points span government and non-government services.
How we went about it:Participants • Advisory group: funding body, U1R agencies, government and non-government stakeholders • 24 agencies participated • Acknowledged concurrent processes and tools: QHIP, CHART and VI-SPDAT • Sector reported that various assessment and data recording processes placed a burden on time • Specialist system uses CHART – no access to CHART for others • Project developed a pre-assessment form (PAF) to link the non-specialist system
How we went about it:The client contact • 116 PAFs were received • 74 were from non-SHS agencies (completing and submitting the whole form) and 42 from SHS agencies (submitting only page three when receiving referrals). • As was expected, more forms were received from Non-SHS agencies because the trial acknowledged that SHS agencies were already conducting assessments via the mandated CHART process and it was decided not to add to work-loads or duplicate effort. • This equated to a total of 74 clients assessed using the PAF. • For the period of the trial - specialist homelessness services participating in the trial recorded 497 entries on chart • Estimates from the non-SHS of homeless people presenting: 403 • 74 is therefore only a sample
How we went about it:Presenting issues: • 25%: Access to accommodation • 24%: Other support relating to homelessness (primarily relating to sustaining tenancies, seeking alternative housing and navigating public and private rental housing) • 18%: financial support (to assist with sustaining tenancy, rent arrears, bill payment, relocation costs, household purchases of emergency relief) • 11%: Access to legal and / or tenancy services Other less frequent primary presenting needs were: • 7%: People in crisis seeking access to immediate supported housing or domestic violence support (4%) • Personal and / or family support - 7% and 4% respectively • Transitional supported accommodation (1%).
What we have learned:Systems design • This project has affirmed the importance of working to develop a Triage System that builds on existing infrastructure and results in recognition for the important and complementary roles of specialist and non-specialist services. • This project occurred at a point in time where other initiatives were maturing such as QHIP and CHART while important innovations like the VI-SPDAT improved capacity to understand and prioritise the needs of highly vulnerable people • The current structure of QHIP and CHART only allows access by the specialist system and this project has identified that a key systems’ change would be to allow integrated access so that the non-specialist system in contact with homeless people can assess people they are in contact with or at least more effectively link to specialist services.
What we have learned:Elements of a triage system • Governance arrangements which harness leadership, and work towards a vision of improved access and outcomes for homeless people • A core role for the specialist homelessness system in both: • Supporting decentralised access points where homeless people naturally present • Directly doing intake and assessment • Directly providing support and accommodation options. • This includes a role for designated specialist services with capacity for ‘hub’ activities including supporting the broader sector, information provision, assessment, referrals and initiating case plans. • Decentralised access points will be valued and recognised as a key way for homeless people to access assistance without taxing their own personal resources.
What we have learned:Overall structure • CHART is proposed as a tool to support and enable triage and that a new or additional tool would add a burden to a system already experiencing high volume • If access to CHART involves delays, then a tool such as the PAF should reflect the content of CHART and be available to the non-specialist system to assess a person and commence a case plan. • A web-based platform for assessments, case planning and ongoing case management and where other key assessments have been done such as a housing application and/or VI-SPDAT, include visibility of these assessments to reduce the burden on clients re-telling their story. • Initial intake and assessment will prioritise people for resources (housing and support) and prioritise a person’s highest, most critical presenting needs as a basis for areas to focus on first. • A case plan commences at the point of triage and moves with the client.
What we have learned:Contextual requirements • A learning and development framework will accompany the triage system with a focus on themes such as assessment, warm referrals, case planning, case coordination and understanding/working with vulnerability across various domains including a focus on mental illness. • A triage system will define various roles including: • Governance • Leadership • Specialist homelessness system hub support • Specialist homelessness system – wider services • Decentralised access points (government and non-government).
Model • Both specialist and non-specialist agencies are important access points for people who are homeless or at risk of homelessness • The non-specialist system can play a role in diverting people from the specialist system and directly to the assistance that a person needs. This system also provides a range of support options that contribute to quality of life. • The specialist system is needed to play a direct role assessing and assisting people, as well as providing specialist support to the wider service system. In that sense it is a direct service provider as well as a systems’ enabler.
So what and what next:The model: • Centralised • Decentralised • Hub and Spoke (centralised support, decentralised access).
jj Source: Under 1 Roof