Download

1 / 46
460 likes | 700 Views
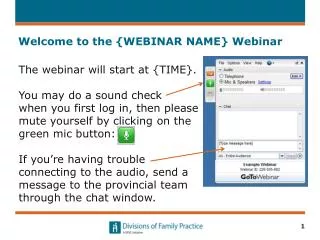
Welcome to the Webinar. Welcome to Trauma Informed Child Welfare: What Does This Mean for Your Work. This webinar is scheduled to begin at 12 :00 PM Eastern, 11:00 AM Central, 10:00 AM Mountain and 9:00 AM Pacific. We will begin shortly.

E N D
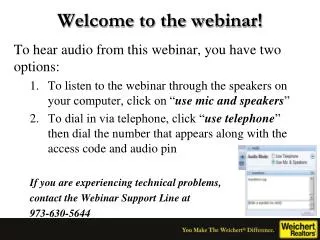
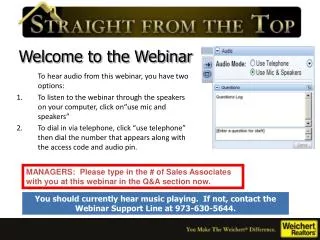
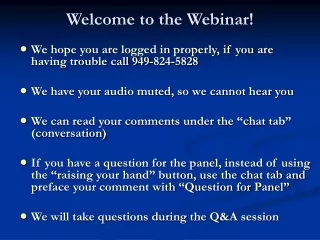
Welcome to the Webinar • Welcome to Trauma Informed Child Welfare: What Does This Mean for Your Work. This webinar is scheduled to begin at 12:00 PM Eastern, 11:00 AM Central, 10:00 AM Mountain and 9:00 AM Pacific. We will begin shortly. • This is a listen only webinar but questions can be asked by typing in the textbox provided on your screen. • If you have any technical difficulties, go to this link to view solutions to common connection problems: http://support.citrixonline.com/en_US/GoToMeeting/help_files/GTM140010?title=Test+Your+GoToMeeting+Connection • The Webinar ID is: 591-244-752
Trauma Informed Child Welfare :What Does This Mean for Your Work? July 23rd, 2013 Julie Collins, MSW, LCSW Director of Standards for Practice Excellence, CWLA
What we will cover • Definition of trauma-informed child welfare • Cover the basics • Trauma and the types of trauma • Impact of trauma • Culture and trauma • Secondary Traumatic Stress (STS) • What a trauma-informed child welfare system looks like • Implications for your work • Resources • Q and A
Different definitions but similar key elements that include the following: a basic understanding of how trauma affects the life of an individual understand the vulnerabilities or triggers of trauma survivors that traditional service delivery approaches may exacerbate assess what can be done to be more supportive, build resilience, and avoid re-traumatization using the “Trauma Lens” Definition of Trauma-informed
A trauma-informed child welfare system is one in which all parties involved recognize and respond to the varying impact of traumatic stress on children, caregivers, families, and those who have contact with the system. Programs and organizations within the system infuse this knowledge, awareness and skills into their organizational cultures, policies, and practices. They act in collaboration, using the best available science, to facilitate and support resiliency and recovery. (as defined by the Chadwick Trauma-Informed Systems Project National Advisory Committee in 2011, Chadwick Trauma-Informed Systems Project, 2013, p. 11).
Essential Elements for Being Trauma-Informed in Child Welfare • Maximize physical and psychological safety for children and families • Identify trauma-related needs of children and families • Enhancing child well-being and resilience • Enhancing family well-being and resilience • Enhance the well-being and resilience of those working in the child welfare system. • Partnering with youth and families • Partnering with child-serving agencies and systems Adapted from NCTSN
What is Child Trauma? • Witnessing or experiencing an event that poses a real or perceived threat to the life or well-being of the child or someone close to the child. Adapted from NCTSN
Situations that can be Traumatic • Child abuse - such as physical, sexual, emotional abuse • Neglect • Witnessing or experiencing community violence • Death or loss of a loved one • Abandonment, betrayal of trust • Life-threatening natural disasters • Acts or threats of terrorism Adapted from NCTSN
Situations that can be Traumatic For Immigrants and Refugees: • War and persecution • Displacement from their home • Flight and migration • Poverty • Family/Community Violence
Child Traumatic Stress • Child traumatic stress refers to the physical and emotional responses of a child to events that threaten the life or physical integrity of the child or of someone critically important to the child (such as a parent or sibling). • Traumatic events overwhelm a child’s capacity to cope and elicit feelings of terror, powerlessness, and out-of-control physiological arousal. Adapted from NCTSN
Child Traumatic Stress • A child’s response to a traumatic event may have a profound effect on his or her perception of self, the world, and the future. • Traumatic events may affect a child’s: • Ability to trust others • Sense of personal safety • Effectiveness in navigating life changes Adapted from NCTSN
Types of Traumas • Acute trauma is a single traumatic event that is limited in time. • Chronic trauma refers to the experience of multiple traumatic events. • Complex trauma describes both exposure to chronic trauma—usually caused by adults entrusted with the child’s care—and the impact of such exposure on the child. Adapted from NCTSN
Types of Traumatic Stress • Historical trauma is a personal or historical event or prolonged experience that continues to have an impact over several generations. • Neglect as trauma is considered a complex trauma that has profound effects on nearly every aspect of a child’s development and functioning. Adapted from NCTSN
Effects of Trauma Exposure Attachment. Children that have been traumatized feel that the world is uncertain and unpredictable. They can become socially isolated and can have difficulty relating to and empathizing with others. Biology. Children that have been traumatized may experience problems with movement and sensation, including hypersensitivity to physical contact and insensitivity to pain. They may exhibit unexplained physical symptoms and increased medical problems. Mood regulation. Children exposed to trauma can have difficulty regulating their emotions as well as difficulty knowing and describing their feelings and internal states. Adapted from NCTSN 14
Effects of Trauma Exposure cont’d Dissociation. Some children that have been traumatized experience a feeling of detachment or depersonalization, as if they are “observing” something happening to them that is unreal. Behavioral control. Children that have been traumatized can show poor impulse control, self-destructive behavior, and aggression towards others. Adapted from NCTSN 15
Effects of Trauma Exposure cont’d • Cognition. Traumatized children can have problems focusing on and completing tasks, or planning for and anticipating future events. • Some exhibit learning difficulties and problems with language development. • Self-concept. Traumatized children frequently suffer from disturbed body image, low self-esteem, shame, and guilt. Adapted from NCTSN
Effects on the Brain Permanent changes in neurochemistry that continue into adulthood can be caused by: early trauma prolonged separation insecure attachment to caregiver(s) (Van der Kolk, 1987)
Emotional/Behavioral Regulation Regulated Definition Maintain Affect, Awareness, Action (3 A’s) over a usual range of stressors Dysregulation of Emotion Definition Shift in Affect, Awareness, Action (3 A’s) over usual range of stressors. Shift in Action does not involve risky/dangerous behavior Dysregulation of Behavior (and Emotion) Definition Shift in Affect, Awareness, Action (3 A’s) over usual range of stressors. Shift in Action does involve risky/dangerous behavior Adapted from Heidi Ellis Trauma Systems Webinar Dec 2012
Why it is Important to Address • If we don’t look for or acknowledge trauma in the lives of children and adolescents, we end up chasing behaviors and limiting the possibilities for change • The behavioral and emotional adaptations that children who have been maltreated make in order to survive are brilliant, creative solutions, and are personally costly.
Childhood Trauma and Other Diagnosis Common diagnoses for children in the child welfare system include: Reactive Attachment Disorder Attention Deficit Hyperactivity Disorder Oppositional Defiant Disorder Bipolar Disorder Conduct Disorder These diagnoses generally do not capture the full extent of the developmental impact of trauma. Many children with these diagnoses have a complex trauma history. 20
Long Term Consequences of Unaddressed Trauma • Homelessness • Prostitution • Delinquency, violence and criminal behavior • Long-term use of services such as health, behavioral health, correctional, and social services systems • Inability to sustain employment • Re-victimization • Inability to parent • Inter-generational transmission of abuse Adapted from NCTSN
Variability in Responses to Stressors and Traumatic Events The impact of a potentially traumatic event is determined by: The objective nature of the event The child’s subjective response to it Something that is traumatic for one child may not be for another Adapted from NCTSN
Variability in Responses Cont’d The impact of a potentially traumatic event depends on several factors, including: The child’s age and developmental stage The child’s perception of the danger faced Whether the child was the victim or a witness The child’s relationship to the victim or perpetrator The child’s past experience with trauma Adversities the child faces following trauma Presence/availability of adults who can offer help and protection Adapted from NCTSN 23
What are Trauma Triggers? • This is something that reminds the person of a traumatic memory. Sometimes referred to as stressors or stimulus • These reminders are not frightening or traumatic. • These are very diverse – could be a person, a smell, a persons posture, tone of voice, color or type of clothes, object, a movie or scene from a movie, etc. • These are often very subtle and hard to detect or anticipate. • The person has an automatic response to the trigger – could be emotional, physical, mental, behavioral. Adapted from NCTSN
What are Trauma Triggers? • Often the person is not aware they are being triggered • Rather, they just feel the intense response – fight, flight or freeze arousal, emotional dysregulation • Often these responses seem irrational • Overreactions • Respond as if happening now • The person can become overwhelmed with their own response Adapted from NCTSN
The Influence of Culture on Trauma • Social and cultural realities strongly influence children’s risk for – and experience of – trauma. • Children with minority backgrounds are at increased risk for trauma exposure and subsequent development of PTSD. • Lesbian, gay, bisexual, transgender, or questioning (LGBTQ) adolescents contend with violence directed at them in response to suspicion about or declaration of their sexual orientation and gender identity. • Immigrant and refugee families often face additional traumas and stressors, especially when they are undocumented. • Children’s, families’ and communities’ responses to trauma Adapted from NCTSN
The Influence of Culture cont’d • Varied trauma response by culture • Necessity to respond to trauma is universal in terms of the physiological and the social responses • Strong cultural identity and community/family connections can enhance a child’s resiliency • Cultural beliefs and values can help or hinder in regard to the child’s reaction to trauma • For example, shame is a culturally universal response to child sexual abuse, but the victim’s experience of shame and the way it is handle Adapted from NCTSN
Historical Trauma • Collective and cumulative emotional wounding across generations. • Cumulative exposure to traumatic events that not only affects an individual but continues to affect subsequent generations. • The trauma is psychological injury held personally and transmitted over generations. Adapted from NCTSN
Historical Trauma cont’d • Cultural trauma: an attack on the fabric of a society, affecting the essence of the community and its members. • Multigenerational/Intergenerational trauma: occurs when trauma is not resolved, subsequently internalized, and passed from one generation to the next. Adapted from NCTSN
Impact of Historical Trauma Definition: The collective emotional and psychological injury both over the life span and across generations, resulting from a cataclysmic history of genocide Dr. Maria Yellow Horse Brave Heart • Effects: Unsettled trauma, Increase of child abuse and domestic violence • Coping Strategies • Psychological - Depression • Suicide: 2x National rate • Behavioral - Alcohol • 5.5x National rate • Medical - Heart disease • 2x National rate http://www.opi.mt.gov/pdf/indianed/Ottenbacher.pdf
Resiliency: Coping and Protective Factors (Cook, Blaustein, Spinazzola, Van der Kolk, 2003) Parental and social support are key mediating factors in determining adaptation to victimization Believing and validating child’s experience Tolerating child’s affect Managing your own emotional response
Resiliency: Coping and Protective Factors Cont’d Other Protective Factors • Positive attachments and connections to emotionally supportive adults • Cognitive and self regulation abilities • Positive belief about oneself • Intelligence • Disposition/temperament • External attributions of blame
Secondary Traumatic Stress (STS) • Results from exposure to trauma experienced by others, often in the workplace • STS symptoms are often indistinguishable from those experienced directly as a response to trauma • Re-experiencing • Avoidance • Hyperarousal • Distress and impairment • STS is often described as an occupational hazard
Other terms used for STS • Compassion Fatigue – conceptually identical to STS – seen as a less stigmatizing term • Vicarious Traumatization – transformation of inner experience of the therapist that comes about as a result of empathic engagement with traumatic material • Burnout – prolonged response to chronic emotional and interpersonal stressors on the job, determined by the dimensions of exhaustion, cynicism, and inefficacy. http://www.cehd.umn.edu/ssw/cascw/events/SecondaryTrauma/PDFs/BrianBride_PPT.pdf
Burnout vs. STS/VT/CF Burnout STS Related to the work environment Extends to work with traumatized populations Exposure to traumatic material is the precipitating factor • Related to the work environment • Extends to work with any difficult population • Workload and institutional stress are the precipitating factors http://www.cehd.umn.edu/ssw/cascw/events/SecondaryTrauma/PDFs/BrianBride_PPT.pdf
Prevalence of STS • Summary of studies show: • Most service providers • experience some symptoms of STS • have low levels of STS • Significant amount of service providers have relatively high levels of STS • CHILD WELFARE = the highest rates of STS http://www.cehd.umn.edu/ssw/cascw/events/SecondaryTrauma/PDFs/BrianBride_PPT.pdf
Impact of STS on Staff Adapted from 2012 CWLA STS Supersession presentation by NCTSN
System-Level Impact Adapted from 2012 CWLA STS Supersession presentation by NCTSN
What about Supervisors? • Not much focus has been given to studying the impact of STS on this group • Studies of child welfare workers where they showed lower levels of STS - supervisors were a mediating factor. Workers reported supervisors used a more action-oriented approach, offered to help address problems and provided visible ongoing support • While supervisors can be helpful in minimizing STS for workers they too need the supports to minimize STS for them. http://www.cehd.umn.edu/ssw/cascw/attributes/PDF/publications/CW360_2012.pdf
Essential Elements for Being Trauma-Informed in Child Welfare • Maximize physical and psychological safety for children and families • Identify trauma-related needs of children and families • Enhancing child well-being and resilience • Enhancing family well-being and resilience • Enhance the well-being and resilience of those working in the child welfare system. • Partnering with youth and families • Partnering with child-serving agencies and systems Adapted from NCTSN
Implications for Your Work • Use the trauma lens in your CRP work • Reviews • Recommendations • Advocacy • Pay attention to and address STS for CRP members
Resources • http://www.nctsn.org/resources/topics/child-welfare-system • http://surveygizmolibrary.s3.amazonaws.com/library/113599/TICWAdminGuide2ndEdMarch2013electronic.pdf • http://surveygizmolibrary.s3.amazonaws.com/library/113599/GuidelinesApplyingTraumaLens1.pdf • www.cachildwelfareclearinghouse.org
Resources • http://www.nctsn.org/sites/default/files/assets/pdfs/sparcs_cultural.pdf • http://www.nctsnet.org/sites/default/files/assets/pdfs/age_related_reactions_to_a_traumatic_event.pdf • http://www.cdc.gov/ace/findings.htm • http://www.childwelfare.gov
A Trauma Survivor “If I could ask for anything, it would be for you to listen and be kind.”
Contact Information • Julie Collins Director of Standards for Practice Excellence CWLA Phone: 202-688-4155 Email: jcollins@cwla.org