STICH II
280 likes | 328 Views
STICH II. Recruitment and data collection progress to date Dr. Alina Andras Database Manager. Surgical Trial in Intracerebral Haemorrhage. STICH II.

STICH II
E N D
Presentation Transcript
STICH II Recruitment and data collection progress to date Dr. Alina Andras Database Manager Surgical Trial in Intracerebral Haemorrhage
STICH II • Funded by Medical Research Council (UK) and now managed by NIHR on behalf of the MRC-NIHR partnership (Efficiency and Mechanism Evaluation (EME) Programme) * • Sponsored by Newcastle upon Tyne Hospitals NHS Foundation Trust • Registered with Current Controlled Trials ISRCTN22153967 * The view and opinions expressed herein are those of the authors and do not necessarily reflect those of the Department of Health
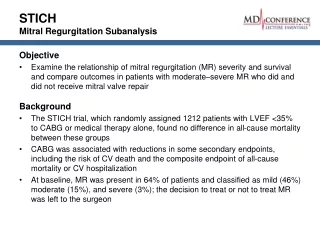
STICH II - Objectives • To establish whether a policy of earlier surgical evacuation of the haematoma in selected patients with spontaneous lobar ICH will improve outcome compared to a policy of initial conservative treatment. • To better define the indications for early surgery.
STICH II Main Features • Multicentre randomised parallel group prospective trial • Spontaneous lobar intracerebral haemorrhage • Treating neurosurgeon must be in equipoise over treatment • 600 patients • Outcome at six months
Europe (55) • Amberg, Germany • Athens, Greece • Berlin, Germany (x2) • Bialystok, Poland • Bilbao, Spain • Borsod County, Hungary • Brno, Czech Republic (x2) • Chisinau, Moldova • Cluj, Romania • Dessau, Germany • Dusseldorf, Germany • Erlangen, Germany • Granada, Spain • Griefswald, Germany • Groningen, Netherlands • Heidelberg, Germany • Istanbul, Turkey • Jena, Germany • Kassel, Germany • Klaipeda, Lithuania • Lübeck, Germany • Liberec, Czech Republic • Magdeburg, Germany • Münster, Germany (x2) • Novosibirsk, Russia • Olomouc, Czech Republic • Ostrava, Czech Republic • Pecs, Hungary • Poznan, Poland • Prague, Czech Republic • Riga, Latvia (x2) • Rome, Italy • Saarbruecken, Germany • Saarland, Germany • Santander, Spain • Siegen, Germany • Skopje, Macedonia • Tbilisi, Georgia • Thessaloniki, Greece (x2) • Timisoara, Romania • Trondheim, Norway • Uppsala, Sweden • Valladolid, Spain • Vienna, Austria • Wiesbaden, Germany • Yerevan State, Armenia Centre Recruitment • Outside Europe (38) • Albany, NY, USA • Bangalore, India • Beijing, China • Bloomington, USA • Calcutta, India • Colombo, Sri Lanka • Dhaklria, India • Dharan, Nepal • Edmonton, Canada • Guadalajara, Mexico • Gwarko, Nepal • Haifa, Israel • Hartford USA • Haryana, India • Hyderabad, India (x2) • Kansas, USA • Kubang Kieran, Malaysia • Lahore, Pakistan • Loyola, USA • Ludhiana, India • Macon, USA • Maharashtra, India • Mansoura, Egypt • Mayo, Jacksonville, USA • Melbourne, Australia • New Delhi, India • Penn State, USA • Peshawar, Pakistan • Riyadh, KSA • Seoul, South Korea • Shanghai, China • Temple, USA • Tianjin, China • Tlalpan, Mexico • Tokyo, Japan • Trivandrum, India (x2) • Vishakhapatnam, India • Zagazig, Egypt Registered Centres 111 Further with Ethics 28 Expressed Interest 99 • UK (18) • Aberdeen • Brighton • Cambridge • Dundee • Edinburgh • Hull • Leeds • Liverpool • London -St George’s • National Hospital • Newcastle upon Tyne • N. Staffordshire • Middlesbrough • Oxford • Preston • Salford • Southampton • Swansea
STICH II patients’ recruitment • Eligibility • Randomisation • Data collection • Randomisation • Two week • CTs • Adverse Events • Outcome
STICH II- Inclusion criteria • Evidence of spontaneous lobar ICH on CT scan (1cm or less from cortex surface) • Patient within 48 hours of ictus • Best MOTOR score on GCS of 5 or 6 and best EYE score on GCS of 2 or more • Volume of haematoma between 10 and 100ml (using Broderick method) • Clinical equipoise
STICH II- exclusion criteria • Clear evidence that the ICH is due to an aneurysm or angiographically proven AVM • Intraventricular haemorrhage of any sort • Hydrocephalus • ICH secondary to tumour or trauma • Basal ganglia, thalamic, cerebellar or brainstem ICH or extension of lobar ICH into any of these regions • Severe pre-existing physical or mental disability or severe co-morbidity that might interfere with assessment of outcome • If surgery cannot be performed within 12 hours
Example 1 This picture shows a scan of a patient who would be eligible for STICH II. The patient has a lobar intracerebral haematoma, close to the cortical surface. The volume of the haematoma is within the 10 – 100 ml criterion. There is no evidence of hydrocephalus or intraventricular haemorrhage and the haematoma does not extend into the basal ganglia, and is not associated with trauma, tumour or aneurysm. Example 2 In contrast this picture shows the scan of a patient who has a haematoma that would exclude them from STICH II. The haematoma is not within 1cm of the cortical surface of the brain. It extends from the lobar region into the basal ganglia. There is evidence also of intraventricular haemorrhage. Example CT scans of patients with intracerebral haematomas that would and would not be eligible for STICH II Included Excluded
STICH II - Recruitment • Patient satisfies criteria • has had a CT scan to confirm the diagnosis, size and location of the haematoma. • Consent or assent obtained • Information sheet is given to patient/relative with time to ask questions • Written witnessed informed consent from • the patient or • the person with the closest personal relationship with the patient who is themselves capable and willing to assent on behalf of the patient. • Copies given to patient and filed in notes and site project file • Complete pre-randomisation record • Web and phone 24 hour randomisation service based in Aberdeen HSRU • Allocation • stratified by country and method of surgery • with a minimisation algorithm based on age group and neurological deficit with a random component
Patient Recruitment:432 patients, 111 centres – 31 March 2011
Recruitment by Centre • 66 out of 111 (60%) centres have recruited at least one patient
Recruitment by Country • Patients have been recruited from 25 countries.
Patient Demographics Age Gender (%) Median Age = 65 years Min = 17 years, Max = 94 years Figures produced for 432 cases
Haematoma Characteristics Volume (ml) Depth (mm from Cortex) Median depth = 1mm Median volume =37 ml Min = 10ml Max = 100ml Side (%) 48% Figures produced for 432 cases 52%
Total GCS at randomisation Median GCS = 13 Figures produced on 31/03/2011 for 432 cases.
Hours to Randomisation Median = 22 hours
Past medical history: • 66% history of hypertension • 47% on anti-hypertensives • 5% previous MI • 10% previous stroke
Medical treatment • At time of ICH • 7% anti coagulants • 11% anti platelet therapy • 1% recent thrombolytic therapy • Following ICH • 1% Factor VII • 11% other coagulants • 26% had an angiogram • 93% no sig vascular lesion, 5% AVM, 3% Aneurysm
Previous functional status: Pre-ICH Rankin Score: Pre-ICH Mobility:
Status at 2 weeks: • 35% Discharged from hospital • 32% Still on neurosurgical ward • 26% Transferred • 7% Dead
Study Flow Chart Initial Conservative Treatment EarlySurgery Diagnostic CT Equipoise Consent to STICH II Telephone randomisation service (24 hours) or web service • 5 Days GCS Monitoring • Day 5 CT • Discharge / 2 week form 6 month outcome questionnaire
Commitments from collaborators • Randomisation forms • CT scans • Discharge/ 2 week follow-up form • (Cross-over forms) • Adverse Event Form • 6 month follow up: • Cover letter • Form • Screening logs
MRC Good clinical trials guidelines • Trial Management Team • Trial Steering Committee • Data Monitoring Committee (DMC) • Ethical Approval and R & D Approval (UK) • Sub agreement
Acknowledgements • Steering and Data Monitoring Committees • All Co-investigators • All patients and carers • Medical Research Council www.research.ncl.ac.uk/stich email: stich@ncl.ac.uk