Download
1 / 84
870 likes | 1.13k Views
Pathology of Glomerular Disease II. Dr. Álvaro Barboza Quintana. Return to Renal Learning Module. Clinico-pathologic Classification in Renal Syndromes. H = High frequency among patients with the syndrome L = Low frequency among patients with the syndrome 1. Nephrotic Syndrome (NS)

E N D
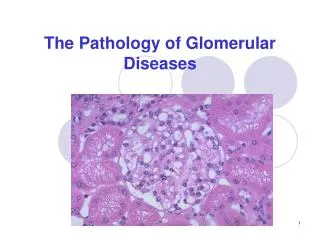
Pathology of Glomerular Disease II Dr. Álvaro Barboza Quintana.
Return to Renal Learning Module Clinico-pathologic Classification in Renal Syndromes • H = High frequency among patients with the syndrome • L = Low frequency among patients with the syndrome • 1. • Nephrotic Syndrome (NS) • Primary Nephrotic Syndrome • Minimal change disease - H • Focal segmental glomerulosclerosis - H • Membranous glomerulopathy - L • Systemic Nephrotic Syndrome • Diabetes mellitus - H • Amyloidosis - L • Systemic lupus erythematosus (WHO Class V)
Minimal Change Disease(Lipoid Nephrosis) • Most frequent cause of nephrotic syndrome in children (2 – 6 years of age). • Follows a respiratory infection or routine prophylactic immunization. • “Its most characteristic feature is its usually dramatic response to corticosteroid therapy” • Etiology: It’s not known, in most cases is idophathic. • Interstitial nephritis by medical treatment • HIV, heroin • Hodgkin disease
Morphology MCD • By light microscopy the glomeruli are normal. • By electron microscopy, the basement membrane appears normal. • Principal lesion: visceral epithelial cells show a uniform, and diffuse effacement of foot processes, • “Fusion” of foot processes, represents simplification of the epithelial cell architecture with flatening, retraction and swelling of foot processes.
Glomeruli are normal by light microscopy in minimal changedisease, as shown in thisbiopsy. The glomerular basement membrane is thin and delicate, and mesangial cellularity andmatrix are within normal limits. (Jones' silver stain, X200).
In this electron micrograph, overlying epithelial cell foot processes are effaced (giving the appearance of fusion) and run together.
Morphology MCD • This changes are reversible after corticosteroid therapy and remission of the proteinuria. • The cells of the proximal tubules are often laden with lipid, reflecting tubular reabsorotion of lipoproteins passing through diseased glomeruli: Lipoid nephrosis. • Immunofluorescence studies show no immunoglobulin or complement deposits.
Clinical Course • Nephrotic syndrome: • Proteinuria (albumin) > 3.5 g/day. • Hipoalbuminemia • Edema • Hyperlipidemia • Lipiduria • Thromboembolic events • Slow decrease of the glomerular filtrate
Membranoproliferative Glomerulonephritis(Mesangiocapillary glomerulonephritis) • 5% to 10% of cases of idiopathic nephrotic sd. In children and young adults (< 30 years). • Associated with other systemic disorders and known etiologic agents (secundary MPGN) or may be primary, without known cause (idiopathic) in the kidney. • Primary MPGN • Type I: Inmune complexes and activation of alternative and classic pathways of complement • Type II:Alternative pathway of complement. Autoantibodies IgG (Nephritic factor C3) which joins with C3 convertase and inactivate C3.
Morphology MPGN • By light microscopy, both types are similar. • The glomeruli are large and hipercelular (by proliferation of cells in the mesangium). • The glomeruli have an “hyperlobular” appearance accentuated by the proliferating mesangial cells and increased mesangial matrix. • The GBM is thickened in the peripheral capillary loops. • The glomerular capillary wall aften shows a “double-contour” or “tram-track” appearance (silver or PAS stains).
As seen here, the glomerulus has increased overall cellularity, mainly mesangial.
Extensive double contours of the glomerularbasement membranes, stained by silver, inmembranoproliferative glomerulonephritis type 1, causedby mesangial interposition and new basement membraneformation in response to subendothelial immune complexdeposits. The deposits are PAS positive andglobular-to-sausage shaped (Jones' silver stain; originalmagnification, x400).
Type I MPGN • 2/3 of cases • “Subendothelial electrodense deposits” under transmission electronic mycroscopy. • Immnunofluorescence • C3 in a granular pattern • IgG • Early complement components (C1q and C4).
Membranoproliferative glomerulonephritis type 1.The marked endocapillary proliferation (proliferatingendothelial and mesangial cells) appears to occlude thecapillary lumen. Numerous large subendothelial andoccasional mesangial-dense immune complex-typedeposits (bottom middle) are present (transmissionelectron microscopy; original magnification, x4,700
Segmental, coarsely granular-to-globular orelongated capillary wall IgG deposits inmembranoproliferative glomerulonephritis type 1(immunofluorescence with anti-IgG; originamagnification, x200).
This electron micrograph demonstrates the dense deposits in the basement membrane of MPGN type II. There are dark electron dense deposits within the basement membrane that often coalesce to form a ribbon-like mass of deposits.
Type I • Clinical Course: Massive proteinuria,Nephrotic sd. • Treatment: Elimination of the infection. • Prognosis: Good, 70 – 85% without clinical alterations. Type II • Clinical Course: Nephrotic and Nephritic sd. • Prognosis: Most patients progress to end-stage renal disease within 10 years. • In both types: Hipocomplementemia, cause of the comsumption in the glomeruli.
Membranous Glomerulonephritis Membranous Nephropathy Epimembranous GN Spikes GN
Membranous GN • Most common cause of nephrotic syndrome in adults. • Characterized by: • Diffuse thickening of glomerular capillary wall • Accumulation of electron-dense, deposits of immunoglobulin. • Along the subepithelial side of the basement membrane
Membranous GN • Idiopathic – 85% of cases • Secondary to: • Drugs: penicillamine, captopril, gold, NSAIDs • Underlying malignant tumors: carcinoma of lung, colon and melanoma. • Systemic Lupus: Most common type. • Infections: chronic hepatitis B/C, syphilis, schistosomiasis, malaria. • DM, thyroiditis.
Early Stage: Glomeruli appear normal or exhibit uniform, diffuse thickening of glomerular capillary wall.
BM material is laid down between the deposits, appearing as irregular spikes protruding from the GBM (silver stain is the best)
IMMUNOFLUORESCENCE: Deposits of immunoglobulines (G or M) and complement.
Electron microscopy: thickening by irregular dense deposits between BM and podocites (subepithelial). Podocites have lost their foot processes.
Clinical Course • Nephrotic syndrome or non-selective proteinuria. • Common symptoms: hematuria, hypertension, and symptoms of secondary causes. • Course: irregular, indolent. • As the glomeruli sclerosis progresses: BUN elevated, hypertension and reduction in severity of proteinuria.
Prognosis and Treatment • Prognosis: • 60% recovers with persistent proteinuria • 10% die or progress to renal insufficiency. • Spontaneous remission and better prognosis in women with non-nephrotic proteinuria. • Treatment: • NON
Amyloidosis • A systemic immune disease characterized by deposition of amyloid (may be localized) • Amyloid is a pathologic proteinaceous substance, deposited between cells in various organs and tissues with a wide variety of clinical settings. • Tipically involves: • Kidneys, spleen, liver, myocardium, adrenals, thyroid, pituitary and tongue. • Associated with:multiple myeloma, chronic inflammatory conditions, chronic renal failure, Alzheimer’s disease, type 2 diabetes.
Amyloidosis • Amyloid is formed by fibril proteins in 95% and by glycloproteins (P component) in 5%. • There are 15 biochemically distinct forms of amyloid proteins: • Amyloid Light Chain • Amyloid –associated protein • Ab amyloid in Alzheimer’s disease • All produce the same consequences and give the same pattern in microscopy.
Renal amyloidosis is the most common and potentially the most serious form of organ involvevement.
Gross Pathology Kidneys may be either : (1)Enlarged, firm with a waxy appearance (2)Shrunken and contracted owing to vascular stenosis.
E A R L Y S T AG E Amyloid is deposited in the glomeruli, interstitium, arteries and arterioles. Appear as irregular thickenings of mesangium and capillary basement membranes.
Congo Red Stain - Polarizing microscopy Show diffuse amyloid deposition (green birefringence) in glomerular tufts and mesangial regions.
END STAGE: Glomerular tufts are flooded and replaced by masses or ribbons of amyloid.
Poststreptococcal Glomerulonephritis(Postinfectious Acute Glomerulonephritis)
Pathogenesis • Secondary to a pharyngeal infección with varying latent period • Nephritic syndrome • Group A (1,2,3,4,12,18,25,49,55,57,60) • Low complement levels, and high titles of streptococcal products. • Glomeruli • Granular immune deposits • Endostreptsin and cationic antigens in afected áreas
Macro • Macroscopic hematuria with a rusty or smokey hue. Micro • Glomeruli: bloodless, hypercelular and enlarged. • Proliferating mesangial and endothelial cells oclude the capillary lumina • PMN and monocyte infiltration. • Exudative and difuse (will affect all the lobules) • Interstitium: edema
Electron Microscopy • Dome-shaped deposits projecting outward from epithelial side of basement membreane. • Epithelial cell slit pores • Separated from the basement membrane by cearl zone continuos with the lamina rara externa. • PMN and monocytes
Clinical Features • Spontaneous nefritic syndrome • Fever, nausea, gross hematuria, oliguria after recovery from pharyngitis. Note: adults have a less spontaneous start with HTA. During epidemics, symptoms may be rare. 1% of children develop intense oliguria and progresive glomerulonephritis. • Outcome in adults is less favorable. • During sporadic cases, 60% have an early recovery. • 1 or more weeks.
Glomeruli show diffuse hypercellularity due to mesangial and endothelial cell increase and a large number of polymorphonuclear neutrophils (PMNs). H&E
Diffuse proliferative acute postinfectious glomerulonephritis with numerous PMNs with PAS-positive cytoplasm and endocapillary proliferation. PAS
The garland pattern of immune complexes due to large subepithelial deposits in acute postinfectious glomerulonephritis is shown (immunofluorescence