Download
1 / 28
1.03k likes | 4.42k Views
Congenital Anomalies of Central Nervous System. Prof Samiya Naeemullah Diplomate American Board Of Pediatrics FCPS,FAAP. Head Of Department Of Pediatrics Islamic International Medical college. Learning Objectives. Recognize Anomalies of Head Hydrocephalus,Microcephaly

E N D
Congenital Anomalies of Central Nervous System Prof Samiya Naeemullah Diplomate American Board Of Pediatrics FCPS,FAAP. Head Of Department Of Pediatrics Islamic International Medical college
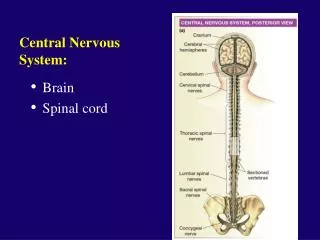
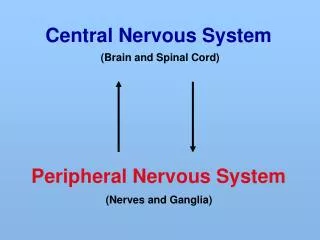
Learning Objectives • Recognize Anomalies of Head • Hydrocephalus,Microcephaly • How do they Present clinically • Recognize anomalies of Spine • Neural Tube defects • Spina bifida • Recognize clinical manifestations
HYDROCEPHALUS • Congenital • Acquired • Excessive accumulation of cerebrospinal fluid (CSF) in the cerebral cavity . • There is either impaired absorption or increased production of CSF. • There Is obstruction to the flow of CSF and dilatation occurs distal to obstruction
Clinical features • IN INFANTS • Accelerated rate of enlargement of head • Anterior fontanel is wide and bulging • Scalp veins are dilated • The forehead is broad • Fixed downward gaze • And sunsetting of eyes
OLDER CHILDREN • Irritability,lethargy • poor appetite • vomiting,headache • A gradual change in personality and intellectual productivity • Serial measurement in head circumference shows increased velocity
EXAMINATION Cracked Pot sign • Papilledema, • Abducens nerve palsy • Pyramidal tract sign more evident in lower limbs
MACROCEPHELY • Head circumference above 98th percentile • Normal children may have large heads • Familial • Tall stature • Hydrocephalus • Subdural hematoma,Cerebral tumour, • Cerebral gigantism
MICROCEPHALY • Head circumference below 2nd centile • Abnormalities in fetal development during neuronal migration • Familial • Autosomal recessive condition with developmental delay • Congenital infection • Perinatal Asphyxia,meningitis
NEURAL TUBE DEFECTS • Failure of the neural tube to close spontaneously between 3rd & 4th week in utero development • CAUSES • Maternal Diabetes • Maternal obesity • Mutations in folate dependent or folate responsive pathways
MAJOR DEFECTS • Spina bifida occulta • Meningocele • Myelomeningocele • Encephalocele • Anancephaly • Dermal sinus • Tethered cord
SPINA BIFIDA OCCULTA • Midline defect of the vertebral bodies without protrusion of the spinal cord or meninges • Mostly asymptomatic • In the midline of the lower back(L5 S1) Patches of hair, Lipoma, Discolouration of skin Dermal sinus • ,
MENINGOCELE • Meninges herniate through a defect in posterior vetebral arches • A fluctuating midline mass that transilluminates occurs along the vetebral column in lower back well covered with skin
MYELOMENINGOCELE • Most severe form of dysraphism • 1 in 4000 live births • Lumbosacral in 75% of cases. • Dysfunction of many organs and structures including skin, skeleton, gastrointestinal and genitourinary tract.
NEUROLOGIC DEFICIT • Depends on the location of defect • Low sacral • Bladder and Bowel incontinence • Mid Lumber Region • Flaccid paralysis of lower limbs • Absent deep tendon reflexes • Lack of response to touch and pain • High incidence of lower extremity deformities.
ANENCEPHALY • A defect in the calvarium meninges and scalp • Rudimentary brain • failure of closure of rostral neuropore (opening of the anterior neural tube.) • The cerebral hemispheres and cerebellum are absent and a residue of brainstem present
PREVENTION • Folic Acid Tablets • 4 mg daily one month before conception