Download
1 / 38
460 likes | 663 Views
Evolving Therapeutic Strategies in Triple Negative Breast Cancer: SABCS 2018 Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California San Francisco Comprehensive Cancer Center San Francisco, CA USA. Topics. Immunotherapy

E N D
Evolving Therapeutic Strategies in Triple Negative Breast Cancer: SABCS 2018 Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California San Francisco Comprehensive Cancer Center San Francisco, CA USA
Topics • Immunotherapy • Current data • New directions • Combinations to enhance host anti-tumor immunity • Early stage disease • Antibody drug conjugates • Reducing toxicity from chemotherapy • Timing of adjuvant chemotherapy
Antitumor Immunity Is a Dynamic Process Trafficking of T cells to tumors Priming & activation Infiltration of T cells into tumors Cancer antigenpresentation Recognition of cancer cells by T cells Release of cancer cell antigens Killing of cancer cells Presented by: Dr. Thomas Powles Chen and Mellman 2013; Liakou et al. 2008; Herr and Morales 2008; Bajorin et al. 2014
PD-1/PD-L1 Blockade in TNBC • Programmed death 1 (PD-1) is upregulated on activated T cells • Inhibits killing by T cells when binds to PD-L1 • PD-L1 expressed on tumor cells or in the tumor microenvironment • Proof-of-concept in metastatic TNBC observed • Monoclonal antibodies target PD-L1 (avelumab, atezolizumab) or PD-1 (pembrolizumab) Ribas A. NEJM 2012; 366:2517-2519
Modest RR with Checkpoint Inhibitor Monotherapy Nanda et al, JCO 2016; Rugo et al, CCR 2018; Dirix et al, BCRT 2017; Loi et al, SABCS 2017; Emens et al, JAMA Onc 2018; Adams et al, Ann Onc 2018 *Studies used different antibodies and cutoffs for PD-L1 positivity
Monotherapy ORR for Metastatic TNBC: Line of Therapy Matters Atezolizumab (n = 115) Pembrolizumab (n =222) 30% 26% 23% 20% Objective Response Rate (%) 10% 6.8% 4.7% 0% 2L+ 1L 1L 2L+ Keynote-086, Cohort B Keynote-086, Cohort A Emens et al, JAMA Onc 2018; Adams et al, Ann Onc 2018
Immunologic Differences Between Primary and Metastatic Tumor Samples PD-L1 + rates (≥1% stromal or tumor cells) Change in PD-L1 status between the primary and metastatic cohorts. Percent TIL counts in full sections and TMAs. Szekely, et al (Pusztai), Ann Oncol 2018
Overall Survival by RECIST Pembrolizumab Atezolizumab N=96 Median OS: 9.3 mo N=81 Median OS: 19.2 mo Adams et al, Ann Onc 2018; Emens et al, Jama Onc 2018
IMpassion130 study design Median follow-up = 12.9 months 1st Interim OS ~ 60% of events occurred • Co-primary endpoints were PFS and OS in the ITT and PD-L1+ populationsd • Key secondary efficacy endpoints (ORR and DOR) and safety were also evaluated • Key IMpassion130 eligibility criteriaa: • Metastatic or inoperable locally advanced TNBC • Histologically documentedb • No prior therapy for advanced TNBC • Prior chemo in the curative setting, including taxanes, allowed if TFI ≥ 12 mo • ECOG PS 0-1 • Stratification factors: • Prior taxane use (yes vs no) • Liver metastases (yes vs no) • PD-L1 status on IC (positive [≥ 1%] vs negative [<1%])c • Atezo + nab-P arm: • Atezolizumab840 mg IV • On days 1 and 15 of 28-day cycle • + nab-paclitaxel 100 mg/m2 IV • On days 1, 8 and 15 of 28-day cycle RECIST v1.1 PD or toxicity R 1:1 Double blind; no crossover permitted • Plac + nab-P arm: • Placebo IV • On days 1 and 15 of 28-day cycle • + nab-paclitaxel 100 mg/m2 IV • On days 1, 8 and 15 of 28-day cycle Schmid P, et al. NEJM 2018
IMpassion130: Nab-paclitaxel +/- Atezolizumab as First-Line Therapy for Metastatic TNBC PD-L1+ populationa ITT population PD-L1+ PFS Stratified HR, 0.62(95% CI: 0.49, 0.78) P < 0.0001 ITT PFS Stratified HR, 0.80(95% CI: 0.69, 0.92)P = 0.0025 5.0 mo(3.8, 5.6) 7.5 mo(6.7, 9.2) 5.5 mo(5.3, 5.6) 7.2 mo(5.6, 7.5) PD-L1+ OS Stratified HR, 0.62 (95% CI: 0.45, 0.86)c ITT OS Stratified HR, 0.84(95% CI: 0.69, 1.02) P = 0.0840b Clinically meaningful PFS and OS benefit in the PD-L1+ population Schmid et al, NEJM 2018 15.5 mo(13.1, 19.4) 25.0 mo(22.6, NE) 17.6 mo(15.9, 20.0) 21.3 mo(17.3, 23.4)
IMpassion130: Efficacy in immune biomarker subgroups from the global, randomized, double-blind, placebo-controlled, Phase III study of atezolizumab + nab-paclitaxel in patients with treatment-naive triple negative breast cancer Emens et al, SABCS 2018 PD-L1 measured by Ventana SP142 PD-L1 IHC assay H&E, Haematoxylin and Eosin In the IMpassion130 study, ~40% of patients had PD-L1-positive tumours1 • Defined as >1% PD-L1 on tumour-infiltrating immune cells
In IMpassion130, PD-L1 in TNBC is expressed mainly on tumor-infiltrating immune cells The majority of patients with expression of PD-L1 on TC are included within the PD-L1 IC+ population PD-L1 TC+ 9% PD-L1 IC+ 41% 34% 7% 2% BEP, biomarker-evaluable population. BEP (TC): n = 900. PD-L1 scoring: IC0: < 1%; IC1: ≥ 1% and < 5%; IC2: ≥ 5% and < 10%; IC3: ≥ 10%; TC–: < 1% PD-L1 on tumor cells; TC+: ≥ 1% PD-L1 on tumor cells. Emens LA, et al. IMpassion130 biomarkers. SABCS 2018 (program #GS1-04)
Biomarker Analysis Pre-treatment biopsies PD-L1 on immune cells and tumor cells using VENTANA PS142 assay Intratumoral CD8+ T cells by IHC BRCA 1/2 by FoundationOne Results PD-L1 IC status predicts PFS and OS benefit with atezo/nab (no benefit in IC negative) PD-L1+ IC are enriched in CD8+; CD8+ are enriched in PD-L1+IC CD8+ only predictive of benefit if IC are PD-L1+ TILS were enriched for PD-L1+ IC Patients with TILS derived benefit only if tumors were also PD-L1 IC+ Benefit from atezolizumab independent of BRCA 1/2 status
I-SPY2: Pembrolizumab Graduated for Efficacy in HER2-Negative Cohorts • Current I-SPY2 Immunotherapy Arms: • Pembolizumab x 8, no AC • Olaparib/Durvalumab/Pac->AC Nanda et al, ASCO 2017
KEYNOTE-173 Schema: Pembrolizumab in early stage TNBC • Endpoint: Safety/tolerability, determine RP2D • 10 patients/cohort Schmid et al, PD5-01, SABCS 2018
KEYNOTE-173 Safety/Efficacy pCR rate with platinum 60% *Met threshold for RP2D Schmid et al, PD5-01, SABCS 2018
KEYNOTE-522 Phase III Trial Pembro 200 mg q3w X 4 cycles+ Carbo (AUC 5 q3w x4 cycles) + Paclitaxel 80 mg/m2 qw 4 cycles (Pembro 200 mg q3w + doxorubicin 60 mg/m2 or epirubicin 90 mg/m2 + cyclophosphamide 600 mg/m2) q3w x4 cycles • 1,174 patients • Locally advanced, centrally confirmed TNBC • T > 2 cm • Bilateral and multifocal BC are allowed • Inflammatory BC is allowed • No chest wall involvement • Dual Primary Endpoints • pCR • EFS • Secondary Endpoints • pCR • EFS • OS • Safety and tolerability Surgery Pembro 200 mg q3w x 9 cycles R Placebo q3w x 4 cycles + carboplatin (AUC 5 q3w x 4 cycles or AUC 1.5 qw x4 cycles) + Paclitaxel 80 mg/m2 qw x 4 cycles Placebo q3w + doxorubicin 60 mg/m2 (or epirubicin 90 mg/m2) + cyclophosphamide 600 mg/m2) q3w x 4 cycles Surgery Placebo q3w x 9 cycles ClincalTrials.gov NCT03036488
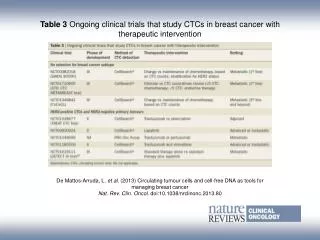
Randomized Ongoing Trials in TNBC (examples) • Metastatic disease (PD-L1 subset analyses) • First line • Pembro + gem/carbo or paclitaxel/nab-P • Atezo + paclitaxel or gem/carbo • Later line • Keynote119: pembrolizumab vs chemotherapy (TPC) (completed accrual) • Neoadjuvant therapy • 2 Phase III trials • Impassion 031: atezolizumab • Keynote 522: pembrolizumab • ISPY 2: • Pembro 8, drop AC in responders • Durvalumab/olaparib + paclitaxel • Adjuvant therapy • SWOG S1418/NRG BR006: post-NAC pembrolizumab • Impassion 030: Atezolizumab • A-Brave: Avelumab post adjuvant chemo (n=355)
TONIC Trial Kok et al, ASCO 2018
InCITe: Innovative Combination Immunotherapy for Metastatic Triple Negative BCTBCRC 047 R A N D O M I Z E R E G I S T E R Binimetinib • Metastatic TNBC • Measurable disease • No more than 3 prior metastatic lines of chemotherapy • Known PD-L1 status • Prior IO allowed Binimetinib +Avelumab Utomilumab +Avelumab Utomilumab PF04518600 PF04518600 +Avelumab Novel agent 1: Binimetinib, a MEK inhibitor Novel agent 2: Utomilumab, a 4-1BB agonist Novel agent 3: PF04518600, an OX40 agonist 1 Cycle=4weeks 15 daylead-in Tumor assessments & PRO q 8wks Tumor biopsy Blood collection Tumor biopsy Blood collection Blood collection (at 8 weeks and at PD) Amulticenter,multi-armTBCRCstudyfundedbytheBreastCancerResearchFoundation
PARP Inhibition May Enhance Immune Surveillance Through Multiple Mechanisms Topacio and Mediola trials indicate safety combining PARPi with IO: subset analysis unclear (Domchek, Vinayak, SABCS 2018)
Topacio Trial • Phase II trial in TNBC • Niraparib and pembrolizumab • Primary endpoint: ORR • 55 patients enrolled, 47 evaluable for efficacy • 19 with clinical benefit (40%) • 10 with BRCA1/2 mutation, 8 with no BRCA1/2 mutation • 4 with other mutations in HRR/DDR Vinayak et al, PD5-02, SABCS 2018
Topacio Biomarker Analysis • 34 samples with TNBC; 15 with CB, 19 without CB • Nanostring to look for differential gene expression • 36 genes differentially expressed in patients with clinical benefit (p<0.05) • PD-1 expression, but not PD-L1 expression, was associated with clinical benefit • Those with clinical benefit had higher T cell inflamed GEP • Those with benefit had higher T cell inflamed GEP regardless of mutation status This presentation is the intellectual property of the author/presenter. Contact hope.rugo@ucsf.edu for permission to reprint and/or distribute.
Mediola Trial • BRCA mutation carriers with metastatic disease, 0-2 prior lines of Rx • Treatment: 4 week olaparib run-in followed by the combination of olaparib and durvalumab • 34 enrolled, 30 evaluable • BRCA1: 15; BRCA2: 15; 13 HR+, 17 TN • 30% no prior therapy for metastatic disease Domchek et al, PD5-04, SABCS 2018
Summary • Difficult to separate efficacy of PARP inhibitor in TOPACIO, BUT responses were seen in tHRR mutants beyond BRCA1/2 and in a small number of patients lacking tBRCA1/2 or tHRR mutations • In MEDIOLA response was similar to that expected with PARP inhibition alone • Need to wait for additional data to understand the impact of addition a CPI to a PARP inhibitor • Paclitaxel, durvalumab and low dose olaparib currently being tested in I-SPY2
Antibody Drug Conjugates Deliver a toxic payload directly to the cancer cell • Receptor binding and internalization
Antibody-Drug Conjugates in Development for TNBC ABT 414: depatuxizimab mafodotin, targets EGFR linked to MMAF 1. Yardley DA, et al. J Clin Oncol. 2015;33(14):1609-1619. 2. Forero-Torres A, et al. Cancer Res. 2017;77(4_Suppl): Abstract P6-12-04. 3. Bardia A, et al. J Clin Oncol. 2017;35(19):2141-2148.
METRIC: Efficacy cape cape Vahdat et al, SABCS 2018
Sacituzumab Govitecan • Linker for SN-38 • Hydrolysable linker for payload release • High drug-to-antibody ratio (7.5:1) • Humanized anti-Trop-2 antibody • Directed towards Trop-2, an epithelial antigen expressed on many solid cancers, including mBC • SN-38 payload • SN-38 more potent than parent compound, irinotecan • In xenograft models, ADC delivers up to 136-fold more SN-38 than irinotecan Kalinsky et al, SABCS 2018
Sacituzumab in TNBC • 110 patients with refractory TNBC: 10 mg/kg IV d1, 8 q21d • 59% ≥4th-line therapy for metastatic disease • 88% mod-strong+ for Trop-2 by IHC in original publication • Adverse events • 25% dose reductions for toxicity • Grade 3/4 neutropenia (41%); alopecia (36%); nausea, vomiting, and diarrhea common (5%-8% grade 3/4) • Response • Median PFS 5.5 mo • Median OS 12.7 mo Complete response (CR) Partial response (PR) Stable disease (SD) Progressive disease (PD) + Continuing treatment as of June 30, 2017 cutoff Grade 3/4 toxicity: Neutropenia: 41%; FN 8% N/V/D: 5/5/8% Alopecia: 36% Bardia A, et al. J Clin Oncol. 2017;35(19):2141-2148. Bardia A, et al. Cancer Res. 2018;78(4 Suppl): Abstract OT2-07-05.
ASCENT Phase III Trial: Almost Accrued January 17, 2019: Breaking news: accelerated approval of sacituzumab delayed. Immunomedics received a complete response letter from the US FDA citing unresolved manufacturing issues. The FDA raised no concerns about the safety or efficacy of sacituzumab govitecan History: summer 2018 FDA inspection uncovered quality control problems incuding a ‘data integrity breach’ which were believed to have been resolved Metastatic TNBC Refractory/relapsed after ≥2 prior SOC chemotherapies for advanced disease OR 1 therapy for patients who progressed within 12 months of completion of (neo)adjuvant therapy Sacituzumabgovitecan (IMMU-132) 10 mg/kg IV, days 1 and 8 every 21 days • Clinical trials number: NCT02574455 • Completing accrual early 2019 Continue treatment until progression N = 328 • Treatment of physician choice • Capecitabine • Eribulin • Gemcitabine • Vinorelbine StratificationFactors • No. of prior therapies • Geographic region • Presence/absence of known brain metastases Primary Endpoint • PFS (Blinded Independent Central Read) Secondary Endpoint • Overall Survival
Sacituzumab in ER+ MBC • Median number of metastatic chemo lines: 2 • Median number of prior metastatic lines: 5 Randomized phase III trial opening in early 2019: 2-4 lines of chemo, at least one hormone therapy/CDK4/6i: Sacituzumab or TPC (Rugo PI) Bardia et al, ASCO 2018
Does Timing of Adjuvant Chemotherapy Affect Outcome? • 687 women with CSI-III TNBC • Surgery followed by adjuvant chemotherapy • Evaluate impact of TTC from surgery • DDFS • OS (similar impact) N=189 N=329 N=115 N=54 Instituto Nacional de Enfermedades Neoplasicas (Lima, Peru) between 2000 to 2014. Morante et al, SABCS 2018
Multivariate Analysis and Conclusions • Adds to the body of data suggesting that time to chemotherapy impacts outcome in early stage TNBC • Provides further support for neoadjuvant chemotherapy as the primary approach for TNBC
The Dawn of Targeted Therapy for TNBC! Thank you!