Download
1 / 138
1.42k likes | 1.82k Views
Cardiovascular Emergencies and 12 Lead EKG’s. Condell Medical Center EMS System ECRN Packet Module III 2007. Prepared by: Sharon Hopkins, RN, BSN, EMT-P. Objectives. Upon successful completion of this program, the ECRN should be able to:

E N D
Cardiovascular Emergencies and 12 Lead EKG’s Condell Medical Center EMS System ECRN Packet Module III 2007 Prepared by: Sharon Hopkins, RN, BSN, EMT-P
Objectives Upon successful completion of this program, the ECRN should be able to: • understand the normal anatomy & physiology of the cardiovascular system • describe anatomical changes to the heart during ischemic episodes • differentiate presentations of patients with cardiorespiratory complaints
–recognize ST elevation on the 12 lead EKG • identify and appropriately state interventions for a variety of dysrhythmias • review discussion of case presentations • successfully complete the quiz with a score of 80% or better
Cardiovascular System • This system is composed of the heart and blood vessels • Delivers oxygenated blood to all cells • Transports hormones throughout the body • Transports waste products for waste disposal • The heart is a pump • right pump is under low pressure • left pump is under high pressure
3 Components of The Circulatory System • Functioning heart • Sufficient blood volume • Intact blood vessels If any one of the above 3 are not working properly, the patient may be symptomatic and could be in need of intervention
Aorta Superior vena cava Left atrium Right atrium Left ventricle Right ventricle
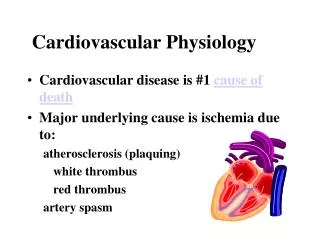
Myocardial Blood Flow • The heart is a muscle (myocardium) • 3 layers • epicardium - smooth outer surface • myocardium - thick middle layer, responsible for cardiac contraction activity • endocardium - innermost layer of thin connective tissue • Myocardial blood flow • via coronary arteries immediately off aorta • heart is the 1st structure to receive oxygenated blood - it’s that important!
Coronary Arteries • Left main coronary artery • left anterior descending coronary artery (LAD) • supplies left ventricle, septum • circumflex coronary artery • supplies left atrium, left ventricle, septum, part of right ventricle • Right coronary artery (RCA) • supplies right atrium & ventricle and part of left ventricle
Collateral Circulation • Development of new blood vessels to reroute blood flow around blockage in a coronary artery • New arteries may not be able to supply enough oxygenated blood to heart muscle in time of increased demand • Ischemia occurs when blood supply to the heart is inadequate to meet the demands
Influences of Heart Function • Preload • pressure under which a ventricle fills; volume of blood returning to fill the heart • Afterload • the resistance the ventricle has to pump against to eject blood out of the heart • the higher the afterload the harder the ventricle has to work • Ejection fraction (EF) • percentage of blood pumped by the ventricle with each contraction (healthy >55%) • damage to heart muscle decreases EF
Afterload arteriosclerosis induced high B/P can cause left ventricle to become exhausted & stop working efficiently Preload increased oxygen demand increases volume of blood returning to heart temporarily not a problem heart enlarges when preload remains increased (Frank-Starling law) Influences On Preload & Afterload
Problems That Decrease Ejection Fraction (EF) • Myocardial infarction (MI) • Congestive heart failure (CHF) • Coronary artery disease (CAD) • Atrial fibrillation • Cardiomyopathy • Anemia • Excess body weight • Poorly controlled blood pressure
Coronary Artery Disease (CAD) • Leading cause of death in USA • Narrowing or blockage in coronary artery decreasing blood flow • Atherosclerosis - thickening & hardening of the arteries due to fatty deposits in vessels • Plaque deposits build up in arteries • arteries narrow • arteries become blocked • blood clots form • Overtime, CAD can contribute to heart failure & dysrhythmias
Coronary Artery Disease (CAD) Plaque in a coronary artery breaks apart causing blood clot to form and blocks artery
Symptoms of Cardiovascular Problems • Breathing problems • Shortness of breath (SOB) • Paroxysmal nocturnal dyspnea (PND) • suddenly awakens with shortness of breath • Orthopnea • dyspnea when lying down • Breath sounds • are they clear or not clear?
Peripheral edema • excess fluid found in tissues of the most dependent part of the body • presacral area in bedridden person • feet and ankles in someone up and about • Syncope • fainting when cardiac output falls • fainting while lying down is considered cardiac in nature until proven otherwise • Palpitations • sensation of fast or irregular heartbeat • Pain
Initial Impression • Not necessarily important to know exactly what to “name” the patient’s problem (diagnosis) • Important to identify signs and symptoms that need to be treated • think “what’s the worse case scenario?” • Important to recognize the possible medical condition the signs and symptoms may be representing • Important to determine the right treatment approach
Patient Assessment:OPQRST of Pain Symptoms • Onset • Sudden or gradual? • Anything like this before? • Provocation or palliation • What makes it better/worse? • What was the patient doing at the time? • Quality • What does it feel like (in patient’s own words)?
Radiation • From where to where? • Severity • How bad is it on a scale of 0-10? • Timing • When did it start • How long did it last? • Continuous or intermittent?
Vital Signs: Tools for Pt Assessment • Heart rate • too fast • ventricle does not stay open long enough to adequately fill • too slow • rate too slow to pump often enough to maintain an adequate volume output • Blood pressure • could be elevated in anxiety and pain • low in shock • serial readings (trending) tell much
Respirations • Abnormally fast, slow, labored, noisy? • Clear - hear breath sounds enter & exit • normal • Crackles - pop, snap, click, crackle • fluid in lower airways • Rhonchi - rattling sounds; resembles snoring • mucus in the airways • Wheezes - whistling sound; initially heard on exhalation • narrowing airways (ie: asthma) • Absence of sound - not good!!!
Pulse oximetry (SaO2) • Measures percent of saturated hemoglobin in arterial blood • <95% indicates respiratory compromise • <90% indicates dire problem • Need to evaluate reading with patient’s clinical presentation - do they match?
Inaccurate SaO2 Readings • Hypotensive or cold patient (falsely low) • Carbon monoxide poisoning (falsely high) • Abnormal hemoglobin (sickle-cell disease) (falsely low) • Incorrect probe placement (falsely low) • Dark nail polish (falsely low) • Anemia (falsely high - whatever hemoglobin patient has is saturated)
EKG monitoring • Indicates electrical activity of the heart • Evaluate mechanical activity by measuring pulse, heart rate and blood pressure • Can indicate myocardial insult and location • ischemia - initial insult; ST depression • injury - prolonged myocardial hypoxia or ischemia; ST elevation; injury reversible • infarction - tissue death • dead tissue no longer contracts • amount of dead tissue directly relates to degree of muscle impairment • may show Q waves
ST depression ST elevation Q wave
Acute Coronary Syndrome Variety of events that represent acute myocardial ischemic pain (plaque rupture) • Unstable angina • Intermediate severity of disease between stable angina and acute MI; tissue ischemia • Non-Q wave infarct (NSTEMI) • No ST elevation but MI is present with tissue necrosis (death) • Q wave infarct (STEMI) • ST elevation MI with tissue necrosis (death) • Usually a large/significant infarct
Acute Myocardial Infarction • Coronary blood flow deprived so that portion of muscle dies • occlusion by a thrombus (blood clot superimposed on ruptured plaque) • spasm of coronary artery • reduction in blood flow (shock, arrhythmias, pulmonary embolism) • Location and size of infarct depends on which coronary artery is blocked & where • left ventricle most common
AMI Signs & Symptoms • Chest pain - most common especially in men • lasts >15 minutes • does not go away with rest • typically felt beneath sternum • typically described as heavy, squeezing, crushing, tight • can radiate down the arm (usually left), fingers, jaw,upper back, epigastrium • Pain not influenced by coughing, deep breathing, movement
Atypical AMI Signs & Symptoms Persons with diabetes, elderly, women, and heart transplant patients • Atypical presentation - from drop in cardiac output (CO) • sudden dyspnea • sudden lose of consciousness (syncope) or near-syncope • unexplained drop in blood pressure • apparent stroke • confusion • generalized weakness
Atypical AMI Signs & Symptoms • Women at greater risk • symptoms ignored (by patient & MD) • under-recognized • under-treated • Typical presentation in women • nausea • lightheadedness • epigastric burning • sudden onset weakness • unexplained tiredness/weakness
Region X SOP Initial Treatment Acute Coronary Syndrome • Regardless of the end diagnosis, all patients treated initially the same • IV-O2-monitor-vital signs-history • aspirin • nitroglycerin • morphine if necessary • 12 lead EKG obtained (transmitted to ED by EMS) • Treatment fine-tuned as more diagnostic information is obtained
Congestive Heart Failure • Heart unable to pump efficiently • Blood backs up into systemic system, pulmonary system or both • Right heart failure • most often occurs due to left heart failure • can occur from pulmonary embolism • can occur from long-standing COPD (esp chronic bronchitis) • Left heart failure • most commonly from acute MI • also occurs due to chronic hypertension
Right Heart Failure • Blood backs up into systemic circulation • gradual onset over days to weeks • jugular vein distension (JVD) • edema (most visible in dependent parts of the body) from fluids pushed out of veins • engorged, swollen liver due to edema • right sided failure alone seldom a life threatening situation • Pre-hospital treatment most often symptomatic • More aggressive treatment needed when accompanied with left heart failure
Left Sided Heart Failure • Heart unable to effectively pump blood from pulmonary veins • Blood backs up behind left ventricle • Pulmonary veins engorged with blood • Serum forced out of pulmonary capillaries and into alveoli (air sacs) • Serum mixes with air to produce foam (pulmonary edema)
Progression Left Heart Failure • Think “left - lungs” • Impaired oxygenation • compensates by respiratory rate • Fluid leaks into interstitial spaces • auscultate crackles • interstitial pressure narrows bronchioles • auscultate wheezing • Dyspnea & hypoxemiapanicrelease of adrenalineincreased work load on heart
Left Heart Failure • Sympathetic nervous system response • Peripheral vasoconstriction • peripheral resistance (afterload) increases • weakened heart has to pump harder to eject blood out through narrowed vessels • blood pressure initially elevated to keep up with the demands and to pump harder against increased vessel resistance • diaphoretic, pale, cold skin
Asthma younger patient hx of asthma unproductive cough meds for asthma wheezing accessory muscles being used Left heart failure older patient poss hx heart problems orthopnea recent rapid weight gain cough with watery or foamy fluid meds for heart problems wheezing JVD Pedal or sacral edema Asthma or Heart Failure?
Which Came First - CHF or AMI? • Not unusual to see the AMI patient in pulmonary edema - watch for it! • Often hard to determine which came first and triggered the development of the other problem • Heart failurepoor perfusion & hypoxemia myocardium suffers from inadequate blood & oxygen supplyacute myocardial ischemiaacute coronary syndrome • AMIpoor pumping performance of heartacute failure of left heart pumpleft heart failure
Cardiogenic Shock • Heart extensively damaged; it can no longer function as a pump • 25% of heart damage causes left heart failure • if >40% of the left ventricle is infarcted, cardiogenic shock occurs • High mortality rate
Signs & Symptoms Cardiogenic Shock • Altered level of consciousness • confusion to unconsciousness • Restless, anxious • Massive peripheral vasoconstriction • pale, cold skin, poor renal perfusion • Pulse rapid and thready • Respirations rapid and shallow • Falling blood pressure
Treatment Goals Acute Coronary Syndrome • Goals • early recognition of a possible cardiac problem • minimize size of infarction • reduce myocardial oxygen demand • decrease patient’s fear & pain (minimizes sympathetic discharge) • salvage ischemic myocardium • prevent development of dysrhythmias • improve chances of survival
Region X SOP - Acute Coronary Syndrome • Oxygen • may limit ischemic injury • Aspirin - 324 mg chewed • blocks platelet aggregation (clumping) to keep clot from getting bigger • chewing breaks medication down faster & allows for quicker absorption • hold if patient allergic or for a reliable patient that states they have taken aspirin within last 24 hours
Nitroglycerin 0.4 mg sl every 5 minutes • dilates coronary vessels to relieve vasospams • increases collateral blood flow • dilates veins to reduce preload to reduce workload of heart • if pain persists after 2 doses, Morphine to be started • Morphine - 2 mg slow IVP • decreases pain & apprehension • mild venodilator & arterial dilator • reduces preload and afterload • 2mg slow IVP repeated every 2 minutes as needed, max total dose 10 mg
Treatment GoalsCongestive Heart Failure • Goals • improve oxygenation • decrease workload of the heart (ie: decrease preload & afterload)
Region X SOPTreatment Stable Acute Pulmonary Edema (B/P>100) • Nitroglycerin - 0.4 mg sl • Vasodilator to create venous pooling • Reduces preload & afterload • Maximum 3 doses (repeated every 5 minutes if blood pressure remains >100) • Consider CPAP - use if indicated
Region X SOP cont’d • Lasix - 40 mg IVP • Diuretic - excess fluid excreted via kidneys • Venodilating effect to pool venous blood • Dose to 80 mg IVP if patient on Lasix at home
Morphine - 2 mg slow IVP • Venodilator to increase pooling of blood • Anxiolytic to calm anxious patient • May repeat 2mg dose every 2 minutes • Maximum total dose 10 mg • Albuterol - 2.5 mg/3ml nebulizer • Wheezing may indicate bronchoconstriction from excessive fluid • Bronchodilator could be helpful
Region X SOP cont’d • Hypotensive side effects from treatments used for stable pulmonary edema • Treatment used (NTG, Lasix, Morphine, CPAP) can all cause venodilation B/P • Blood pressure needs to be carefully monitored
Region x SOP Treatment Unstable Acute Pulmonary Edema (B/P<100) • Contact Medical Control • CPAP on orders of Medical Control • Consider Cardiogenic Shock Protocol • If wheezing (indicating bronchoconstriction), contact Medical Control for Albuterol order • if patient needs to be intubated, Albuterol to be delivered via in-line