Download
1 / 25
260 likes | 1.1k Views
Spontaneous Pnemothorax. Caitlin Darby April 9, 2013 Florida Hospital Tampa. Objectives. Discuss the pathophysiology of a pneumothorax Discuss the types of pneumothorax’s Discuss the risk factors for a pneumothorax Describe the signs and symptoms of a pneumothorax

E N D
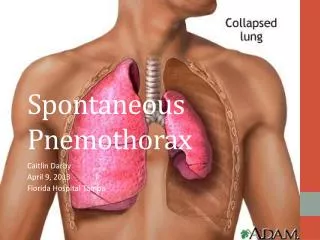
Spontaneous Pnemothorax Caitlin Darby April 9, 2013 Florida Hospital Tampa
Objectives • Discuss the pathophysiology of a pneumothorax • Discuss the types of pneumothorax’s • Discuss the risk factors for a pneumothorax • Describe the signs and symptoms of a pneumothorax • Discuss the prevalence and prognosis of a pneumothorax in our society • Describe the complications and prevention of a pneumothorax • Discuss medical and nursing interventions for a pneumothorax • Describe a patient case scenario • Describe patient outcomes from interventions used in the hospital • NCLEX review questions
Pathophysiology • Air leaks into the space between your lungs and chest wall (pleural space). This air pushes on the outside of your lung and causes it to collapse. • In most cases, only a portion of the lung collapses • Not due to trauma • Exact cause is unknown *
Types of Pneumothorax’s • Spontaneous Pneumothorax • Open Pneumothorax • Closed Pneumothorax • Tension pneumothorax • Hemothorax • Chylothorax *
Risk Factors • First Spontaneous Pneumothorax • Smoking • Causes small airways and risk increases with length of time and number of cigarettes used • Age • Most likely to occur between ages 20-40 • Doesn’t typically affect anyone over 40 • Sex • Men who are tall and thin are more likely than women • Pneumocystis carinii pneumonia (PCP)
Risk Factors (cont.) • Secondary Spontaneous Pneumothorax • A history of pneumothorax • One pneumothorax increases your risk to have another within 2 years • Obstructive lung disease • Ex. COPD • Infectious lung disease • Ex. Tuberculosis • Interstitial lung disease • Ex. Sarcoidosis • Connective tissue disease • Ex. Rheumatoid arthritis
Symptoms • Symptoms • Dyspnea upon exertion • Sudden onset of chest pain on the affected side (unilateral) • Shoulder pain • Shortness of breath • Dry cough • Anxiety • Clicking sound over the front of the thorax
Signs • Signs • Anxious appearance • Asymmetrical chest expansion • Cyanosis • Tachycardia • Hypotension • Increased respiratory rate • Diminished or absent lung sounds on the affected side • Hyper resonance upon percussion • Mediastinal displacement (occasionally with a tension pneumothorax)
Complications of a Pneumothorax • Recurrence • Usually within three years of the first • Highly likely after first occurrence • Persistent air leak • Air may continue to leak if the opening in the lung wont close • Surgery may be needed to close the leak. • Chest x-ray confirms • Sign: bubbling in the water seal chamber
Prevalence in the United States • Primary Spontaneous Pneumothorax • Between 7.4-18 cases per 100,000 population per year among men • Between 1.2-6 cases per 100,000 population per year among women • Approximately 20,000 new cases of a spontaneous pneumothorax are diagnosed each year
Prognosis • Death from a spontaneous pneumothorax is very rare • Mortality rate • 1.26 per million a year for men • 0.62 per million a year for women • Rates of recurrence are high in the United States, finding a total recurrence rate of 35%
Prevention of a Pneumothorax • Smoking cessation • Controlling lung diseases • Follow up chest x-rays every 4-6 months to monitor for recurrence
Medical Interventions • From current research • Antibiotic therapy • Chest x-ray • CT scan • Thorascopy • Needle aspiration • Heimlach valve placement • Chest tube placement (thoracostomy) • Oxygen therapy • Breathing treatments • Daily blood tests (ABG’s, BMP, CBC) • Prescription for pain medication • Telemetry monitoring • Thoracotomy • Resection of lung lesions • Partial or complete parietal pleurectomy *
Case Study • The patient is a 48-year-old male who complains of severe chest pain, difficulty breathing, shortness of breath and coughing. He stated that he had been having these symptoms since February 9, 2013. The patient stated that his symptoms were constant throughout the day and interfered with his daily routines. He described his chest pain and other symptoms as sharp, stabbing, aching, and as though he couldn’t catch his breath. The patient stated that his symptoms were worse upon exertion. The patient tried tums, Motrin and his albuterol inhaler to try and relieve his symptoms. He stated that nothing relieved or lessened his symptoms and that his pain did not radiate to anywhere else in his body. When asked to describe the severity of his symptoms on a scale of 0-10 he reported the intensity as a 5/10. The patient was hospitalized on February 19, 2013 where he underwent treatment for a right pneumothorax including a thorascopy with bleb resection, chest x-rays, CT scan, chest tube placement and breathing treatments.
Patient Scenario • Subjective Findings (symptoms) • Chest pain • Difficulty breathing • Shortness of breath • Non-productive cough • Objective Findings (signs) • Dyspnea • Pallor • Dry cough • Anxiety • Medications • Albuterol • Enoxaparin • Ketoconazole • PredniSONE • Ondansetron • HYDROmorphone • OxyCODONE/acetaminophen
Medical Interventions • Used in the hospital • Thorascopy with bleb resection • Incentive spirometry (Q1H) • Continuous telemetry monitoring • Abdomen x-ray (flat & upright) • Antibiotic therapy • Supplemental oxygen • Analgesic therapy • Bronchoscopy • CBC and BMP lab draws daily • Arterial blood gases • Daily chest x-ray’s • Computed tomography scan • Chest tube placement *
Nursing Interventions • Used in the hospital and from current research • Incentive spirometry use • Monitoring vital signs, breathing pattern, rate, effort and use of accessory muscles every 2 hours • Monitor O2 saturation, daily labs and arterial blood gas results • Assess for changes in mental status, skin color and cyanosis • Administer medication and antibiotics as prescribed • Control the patients pain and anxiety with pharmacological and non pharmacological techniques • Provide oxygen therapy and breathing treatments as needed • Turn and reposition the patient Q2H and position in fowlers or semi-fowlers position (30-45 degrees) to promote expansion of the lungs • Have patient do turn, cough and deep breath exercises and pursed lip breathing exercises every hour • Auscultate lung fields every hour to observe for the return of lung sounds or to note any changes • Record the time and amount of drainage from the chest tube daily • Perform chest tube dressing changes daily promoting a tight seal • Observe for bubbling and fluctuations in the water seal chamber of the drainage system • Ensure chest tube tubing is coiled on the bed with no dependent loops • Monitor results of diagnostic testing *
Diagnostic Tests/Labs • Non-Laboratory tests • Chest x-ray • Computed tomography scan (CT scan) • Abdominal x-ray • Thorascopy • Laboratory tests • Complete blood count (CBC) • Basic metabolic panel (BMP) • Arterial blood gases *
Patient Outcomes • The patients pain level was reduced from a 5/10 to a 3/10 after administration of analgesics • The patients chest x-ray results showed a small air leak when coughing • The patients lung sounds returned post chest tube insertion • The patients BMP, CBC and ABG’s came back within normal range • The patient was resting comfortably with HOB at 30 degrees • The patient was not discharged during my shift
Nursing Diagnosis • Ineffective breathing pattern r/t chest pain a.e.b dyspnea and patient feeling breathless • Anxiety r/t threat to or change in health status a.e.b expressed concerns and restlessness • Acute pain secondary to pneumothorax a.e.b. patient stating pain of a 5/10 and facial grimacing when changing positions • Impaired coping r/t inadequate opportunity to prepare for stressors a.e.b lack of assertive behavior and change in usual communication patterns • Risk for infection r/t inadequate primary defenses a.e.b surgical procedure
NCLEX Question #1 • Which treatment should a nurse expect for a client with a spontaneous pneumothorax? • A. Antibiotics • B. Bronchodilators • C. Chest tube placement • D. Hyperbaric chamber
NCLEX Question #2 • Which method is the best way to confirm the diagnosis of a pneumothorax? • A. Auscultate for breath sounds • B. Have the client use an incentive spirometer • C. Take a chest x-ray • D. Stick a needle in the area of decreased breath sounds
References • Horne, N.W. (1966, January 29). Spontaneous pneumothorax: diagnosis and management. British medical journal, 281-284. Retrieved from http:// www.ncbi.nlm.nih.gov/pmc/articles/PMC1843468/?page=1 • Huether, S., McCanee, K. (2012). Understanding pathophysiology. • Mayo clinic staff. (2011, April 5). Pneumothorax. Mayo foundation for medical education and research. Retrieved from http://www.mayoclinic.com/ health/ pneumothorax/DS00943 • Nursing, C. (2011). Spontaneous pneumothorax. Retrieved from http:// nursing.unboundmedicine.com/nursingcentral/ub/view/Tabers-Dictionary/762378/6/ pneumothorax • Osborne, K.S., Wraa, C.E. &Watson, A.B. (2010). Medical –Surgical Nursing: Preparation for Practice. 988-999. • Rivas de Andres, J., Jimenez Lopez, M., Lopez-Rodo, L., Trullen, A., & Lanzas, J. (2008). Guidelines for the diagnosis and treatment of spontaneous pneumothorax. Recommendations of the spanish society of pulmonology and thoracic surgery, 44(8), 437-448. Retrieved from http:// www.sciencedirect.com.ezproxy.hsc.usf.edu/science/article/pii/ S1579212908600774 • Student Nursing Study Blog. [Web post]. Retrieved from http://amy47.com/nclex-style- practice-questions/airway-pneumonia-and-tb/ • Tschopp, J.M., Rami-Porta, R., Noppen, M., & Astoul, P. (2008, September). Management of spontaneous pneumothorax: state of the art. European respiratory journal, 28(3), 637-650. Retrieved from http://erj.ersjournals.com/content/28/3/637.full http://web.ebscohost.com.ezproxy.hsc.usf.edu/dynamed/detail? vid=3&sid=1f0ab461- c536-467c-b646