CNS Pathology
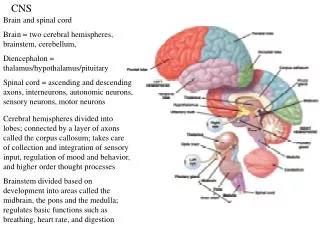
CNS Pathology. Fall 2009 Final. INFLAMMATORY DISEASE OF CNS. Meningitis. Inflammation fo the meningeal coverings of the brain and spinal cord Can be caused by Bacteria, virus and other organisms via blood or lymph Trauma, pentrating wounds or adjacent structures infected

CNS Pathology
E N D
Presentation Transcript
CNS Pathology Fall 2009 Final
Meningitis • Inflammation fo the meningeal coverings of the brain and spinal cord • Can be caused by • Bacteria, virus and other organisms via blood or lymph • Trauma, pentrating wounds or adjacent structures infected • Bacterial is most common (can cause hydrocephalus)
Pathogens causing Meningitis • ___________________ • Chronic meningitis • Often associated with AIDS and immunodepressant drug therapy • ___________________ • Viral meningitis can be caused by mumps, poliovirus and herpes simplex • ___________________ • Most common • Bacteria release toxins that destroy meningeal cells stimulating immune & inflammatory reactions
Pathogens causing Meningitis • Fungi • Chronic meningitis • Often associated with AIDS and immunodepressant drug therapy • Virus • Viral meningitis can be caused by mumps, poliovirus and herpes simplex • Bacteria • Most common • Bacteria release toxins that destroy meningeal cells stimulating immune & inflammatory reactions
Acute Meningitis Clinical Symptoms • Fever • Headache • Stiff neck • Vomiting • Changes in LOC • Severely ill in 24 hours • Rash • Chronic symptoms are the same but occur over weeks
Diagnosis of Meningitis • Brain CT • Rule out contraindications to do a spinal tap • Spinal tap • LP to remove CSF to send to lab • Sometimes MRI is used • Is most sensitive modality for demonstrating pia and arachnoid • Treatment includes: • antibiotics and if secondary to encephalitis: antiviral drugs
Radiographic Appearance • Initially meninges show vascular congestion, edema and minute hemorrhages • MRI and CT scans could appear normal if appropriate therapy is done right away Meningitis as a result of a Staph infection
Encephalitis • Infection of the brain tissue that is viral • May occur subsequent to chickenpox, small pox, influenza and measles • May be caused by mosquitoes and herpes • Survival rates depend of cause of the disease (can be fatal) • 30% of cases in children • When caused by herpes it is often fatal
Encephalitis • MRI is modality of choice • Results in cerebral edema and hemorrhagic lesions • More serious than meningitis because it frequently develops permanent neurologic disabilities
Symptoms: Headache Malaise Coma Fever Seizures Treatment: Treated with antiviral medications Herpes induced is treated with Acyclovir Interferes with DNA synthesis and inhibits viral replication Encephalitis:Symptoms and Treatment
Spinal Bifida • Is a congenital disease • Bony neural arch that not completely closed • Most common in lumbar region • May or may not herniate through opening • Can range in risk from treatable to life threatening • Can be diagnosed in utero • With amniocentesis • Ultrasound • Elevated beta fetoprotein in mother’s blood
Types of Spinal Bifida • ________________ • Only the meninges protrude • Local defect of bone & dura • ________________ • Protrusion of spinal cord • ________________ • Protrusion of meninges and spinal cord into the skin of the back • Most serious • ________________ • No protrusion of spinal contents • Least severe
Types of Spinal Bifida • Meningocele • Only the meninges protrude • Local defect of bone & dura • Myelocele • Protrusion of spinal cord • Meningomelocele • Protrusion of meninges and spinal cord into the skin of the back • Most serious • Spinal bifida occulta • No protrusion of spinal contents • Least severe
Radiographic Appearance Meningomyelocele • Can be demonstrated with CT, MRI and myelography • Prenatally with ultrasound (in utero) • Large bony defects • Herniated spinal contents Meningocele
Meningomyelocele • Most serious • Affected PT’s have severe neurologic deficits • Paraplegia • Diminished control of lower limbs, bladder and bowels • Hydrocephalus is common
Spinal Bifida Treatment • Can be surgically repaired • Neurological damage is permanent still and cannot be reversed • Most measures are supportive rather than corrective • Physical therapy • Physical supports • Braces • Splints
Cranial Fractures • Cerebral fractures usually occurs to fractures of the calvaria of the skull • 3 types of cranial fractures • _____________- straight and sharply defined • Is 80% of all cranial fractures • _____________- curvilinear density • _____________- Air fluid levels are indicative • Hard to diagnosis radiographically
Cranial Fractures • Cerebral fractures usually occurs to fractures of the calvaria of the skull • 3 types of cranial fractures • Linear- straight and sharply defined • Is 80% of all cranial fractures • Depressed- curvilinear density • Basilar- Air fluid levels are indicative • Hard to diagnosis radiographically
Cranial Fractures • Location of FX is more important that the extent of the FX • If FX crosses artery a bleed can occur causing a hematoma • Fx that enters mastoid air cells or sinus can cause an infection that can result in • Meningitis • Encephalitis
Linear Fractures • Non branching lines that are intensely radiolucent • Vascular markings are occasionally mistaken for fractures • Fracture appears more translucent and transverses the full thickness of skull • Sutures
Depressed Fracture • The fractured edges overlap • Usually caused by a high velocity impact with a small object • Can cause bleeding into subarachnoid space • Best demonstrated with CR tangential to the FX
Basilar Fracture • Very difficult to demonstrate with x-ray • Air fluid levels in sphenoid sinuses • Clouding of mastoid air cells • Often X-table lateral is done to demonstrate this • CT & MRI are most often used for this type
Compression Fracture of spine • Most frequent type of injury involving vertebral body • Generally occurs in T and L-spine • T11- T12 and T12 – L1 • Damage is usually limited to the upper portion of the vertebral body, particularly to the anterior margin
Hangman’s Fracture • FX of the arch of the 2nd c-spine vertebrae • Usually accompanied by anterior subluxation of the 2nd and 3rd cervical vertebrae • Sometimes called traumatic spondylosis • Resulting from acute hyperextension of the head & neck • Originally seen commonly in hangings • Now seen more for MVA
Jefferson’s Fracture • Comminuted FX of the ring of the atlas • First described as a “burst FX” • Generally occurs as a result of severe axial force such as a MVA • With this FX particular attn needs to be paid to the transverse longitudinal ligament by reviewing lateral masses on the open mouth odontoid • MRI is preferred method for this ligament
Jefferson’s Fracture
Cerebral Contusion • Is an injury to the brain tissue caused by a movement of the brain within the calvaria after blunt trauma • Occurs when brain contacts rough skull surfaces such as orbital floor and petrous ridges
CT appearance of Cerebral Contusion • CT scans appear as low density areas of edema and tissue necrosis • When IV contrast is used it will enhance several weeks after injury • Plays an important role in diagnosis
MR of Cerebral Contusion • Cerebral edema causes high signal intensity on T2 scans • T1 scans may produce high signal regions • Diagnosis can also include CT, MRI and PET
Clinical symptoms: Drowsiness Confusion Agitation Hemiparesis Unequal pupil size Treatment: PT is hospitalized Prevent shock If there is swelling medication is given to decrease cranial pressure Control edema Drainage of hematoma Surgery is usually not necessary Cerebral Contusion
Hematomas • Brain trauma often resulting in a hemorrhaging from a ruptured vein or artery • Skull does not allow for expansion and pressure forces brain toward open space (foramen magnum) • Can result in major consequences & death if not treated quickly
Epidural Hematomas • Highest mortality relate of the hematomas • Even when treated quickly mortality rate is 30% • Results from a torn artery and its branches • Most often occurs from a FX of the temporal bone • 80% of cases conventional radiograph shows fracture • Usually meningeal artery with blood pooling between bones of the skull & dura mater
Epidural Hematoma Usually a shift of midline Toward opposite side CT shows increased density Emergency surgical decompression is required to relieve cranial pressure
Subdural Hematomas • Between the dura mater & arachnoid meningeal layers • Caused by blunt trauma to frontal or occipital lobes and can tear subdural veins • Pushes brain away from skull across midline (including ventricles)
Subdural Hematoma Occurs more slowly Because it is a venous Hemorrhage. On CT appears as a curvilinear area of I increased density on portions or all of the cerebral hemispheres
Subdural Hematomas • Subacute stage (up to several days) • Appears on CT as a decreased density or isodense fluid collection • In chronic state (2-3 weeks) • The surface of the hematoma becomes concave • Delayed coma con occur
Symptoms of Hematomas • Headaches • Agitation • Drowsiness • Gradual radiograph deficits