Download
1 / 45
450 likes | 609 Views
Minnesota’s Alternative Demonstration for People with Medicare and Medicaid Special Needs Plans and Integrated Care System Partnerships 2013 Age and Disabilities Odyssey June 18, 2013. Pamela Parker, MPA Special Needs Purchasing Minnesota Department of Human Services Pam.parker@state.mn.us

E N D
Minnesota’s AlternativeDemonstration for People with Medicare and MedicaidSpecial Needs Plans and Integrated Care System Partnerships2013 Age and Disabilities OdysseyJune 18, 2013 Pamela Parker, MPA Special Needs Purchasing Minnesota Department of Human Services Pam.parker@state.mn.us 651-431-2512
OVERVIEW • Why Integrate Medicare and Medicaid • Minnesota’s Integrated Programs and Results • History of Integration • New CMS Integration Initiatives and Challenges • Finding the Best Platform for Integration • Status of MN Dual Demo for Seniors and People with Disabilities • Minnesota’s Payment and Delivery Health Reform Initiatives • Integrated Care System Partnerships (ICSPs) • Clinical Measurement for ICSPs • Summing Up
Why We Need Medicare/Medicaid Integration for People with Dual Eligibility • Without partnering with Medicare, States can do little to impact preventive, primary, acute care and post acute care and costs.. • Decisions made by primary, acute and post acute care providers paid under Medicare also drive State Medicaid and LTSS costs. • Care for people with dual eligibility is fragmented and not optimal. • Services to the 10 million people with dually eligibility make up more than a third of all Medicare and Medicaid expenditures and are expected to increase disproportionately. • Shared State and Federal goal to improve care quality and make care more seamless, appropriate and accessible for people with dual eligibility is an imperative. • Combining Medicare/Medicaid primary, acute and LTSS financing in aligned contracts is necessary for creation of provider level payment incentives that can improve care and costs across settings and financing sources. • CMS Medicare-Medicaid Coordination Office (MMCO) is sponsoring new opportunities for States to tackle these issues through demonstrations to align Medicare and Medicaid.
Integrated Programs in MN • Medicaid managed care since 1985, about 600,000 total enrollees. About 88,000 elderly and disabled included. Seniors since 1983, people with disabilities since 2001. • 90% of seniors (49,000) enrolled in managed long term care, includes all home and community based and behavioral health services. 70% of seniors enrolled in FIDE SNPs. Average age 80. 70% eligible for LTSS. • Two options: • Minnesota SeniorCare Plus (MSC+): 12,500 seniors in same 8 Medicaid MCOs, mandatory enrollment unless enrolled in MSHO, Medicare largely FFS. • Minnesota Senior Health Options (MSHO): 36,500 dual seniors in 8 fully integrated Medicare/Medicaid FIDE SNPs, voluntary alternative to mandatory enrollment in MSC+
Integrated Programs in MN • 43% of people with disabilities (39,500) enrolled in Special Needs BasicCare sponsored by 5 Medicaid Managed Care Organizations (MCOs), LTSS carved out, all behavioral health included. • Only 3% in 3 integrated SNPs, 5 other SNPs dropped Medicare SNP for disability group. • MSHO now moving back to Medicare/Medicaid Demonstration status under new CMS demonstration parameters. • Also pursuing separate Demonstration for people with disabilities • Will describe that briefly but not the focus of this presentation
Results Indicators for MSHO Seniors • Contract Requirements for Care Coordination: All members are assigned individual care coordinators. The State sets uniform standards, audit protocols and criteria for assessment, care plans and care coordination. Audit reports, independent onsite reviews and corrective actions are used to follow up. • Encounter Data Analysis: Shows annual assessment and individualized care coordination has significantly increased access to HCBS. • AARP Scorecard: MN has been #1 for HCBS Access. Medicaid long term care for seniors has been rebalanced since the start of managed LTC programs (Sources: 1996 Medicaid Forecast, July 2012 Medicaid enrollment by living arrangement). • Nursing home admissions average about 7% across the senior programs with an average length of stay of about 150 days per year. • About 41% of nursing home admissions return to the community. • About 60% of all EW expenditures are for Assisted Living which is by far the largest single EW service expenditure
Results Indicators for MSHO Seniors • HEDIS: 98% of MSHO seniors have annual primary care visits. • Dual Data Base: Despite much higher chronic disease rates, acute care hospital admits/episode rates for community seniors by risk adjusted categories are lower in MSHO than for regular Medicare members in FFS or other Medicare Advantage. (Source: JEN iMMRS-MN) • STARS: MSHO D-SNPs have had average Star ratings of 4.0 Stars (2012) • CAHPS: MSHO is highest rated Medicaid program. Includes care coordination questions • Disenrollment Rates: Despite voluntary enrollment, MSHO disenrollment is < 2%. • Payment Incentives: Contracts include significant payment withhold tied to timely assessment, financial incentives for provision of LTSS and Health Care Home (HCH) payment flexibility
History of Integration Efforts 1970-1990: Formation of On-Lok and PACE 1985-2007: Social HMO Demo (transitioned to SNPs in 2007) 1987: Evercare begins in MN 1980s: MN Managed Care contracts include Medicare/Medicaid services to duals through Medica/Evercare and Health Partners/Social HMO 1991: First MN proposal to CMS for integrated Medicare and Medicaid program for people with dual status, two more proposals follow 1995: CMS approves first State “Dual Demo” in MN 1997-2004: Two additional State Demos implemented in WI and MA
History of Integration Efforts 2005: CMS requires the 3 State Dual Demos to transition to D-SNP 2010: ACA provides additional authority to CMS for new Medicare-Medicaid Coordination Office (MMCO) to align Medicare/Medicaid for people with dual status 2011: CMS awards 15 states planning contracts for new dual demos 2011: CMS issues Capitated and FSS Financial Alignment Demo (FAD) opportunities to States beyond the original 15 states, 36 States respond 2012-13: OR, MN, HI, TN and AZ drop out of FAD 2013: CMS approves FAD MOUs for MA, WA, IL, OH, CA, VA
The Impossible Dream: CMS MMCO Dual Demo Challenges • Set consistent national standards on key elements but allow flexibility to accommodate State variations • Make Medicare and Medicaid bureaucracies do something different at both Federal and State levels • Resolve innumerable devilish operational details for both Medicare and Medicaid at both State and CMS levels • Meet high and often conflicting expectations and demands from Congress, MedPAC, 30+ States, multiple consumer and provider stakeholders, plans and financial investors! • Manage tensions around Federal vs State control
CMS MMCO Dual Demo Challenges • Evaluate results in 3 years and meet CMS standards for rapid cycle improvement potential • Achieve significant enrollment and significant savings • Position demos for potential permanent platform • Chart course for dual demos among many competing FFS based provider initiatives as well as ongoing Medicare Advantage/Part D competition • CMS MMCO has done astonishing work but this is a gargantuan task, the biggest challenges lie ahead!
Status of State Integration Efforts Medicaid Managed LTSS Only AZ, HI, KS, NM, PA, TN Both Medicaid Managed LTSS and Medicare-Medicaid Care Coordination Initiative CA, DE, FL, IL, MA, MI, MN, NH, NJ, NY, NC, OH, TX, WA, WI Medicare-Medicaid Care Coordination Initiative: *: Financial Alignment (FA) demonstration proposal approved by CMS **: Initiatives other than FA demonstration W: No longer pursuing FA demonstration AZ(W), CA*, CO, CT, DE, FL**, HI(W), ID, IL*, IA, IN**, MA*, MI, MN(W)**, MO, NH**, NJ**, NM(W), NY, NC, OH*, OK, OR(W), RI, SC, TN(W), TX, VA*, VT, WA*, WI Source: NASUAD Integration Tracker May 2013 http://www.nasuad.org/medicaid_integration_tracker.html
Still Searching for the Right Platform • PACE: Enrollment limited to community “nursing home certifiable”, staff model means changing doctors, expensive and inflexible care coordination model • SNPs: Lack of operational alignment with Medicaid, lacks direct communications/role for State, constant conflicts with state policy around enrollment, procurement timelines, quality reporting, assessment timelines, grievance and appeals, marketing, etc. • FAD: Key states (OR, MN, AZ, TN, NM, HI) with large MLTSS programs and/or high degrees of SNP integration dropped out for financial and administrative reasons • MedPAC: New recommendations to give integrated SNPs permanent status and facilitate more integration • Many states still working with SNP based models • All 5 approved Dual Demos have delayed most enrollments to 2014
Non-Integrated SNP Features Separate assessments and Models for Care (MOC) for Medicare and Medicaid Misaligned enrollments Two enrollment forms to sign Separate accretion and deletion dates Two cards and sets of member materials, provider directories, etc. Separate reviews of member materials, State vs RO Two sets of notices (likely misleading) Separate PIPs and QI Typically must have Medicare denial or appeal before Medicaid service picks up May handle claims twice, once for Medicaid, once for Medicare Providers normally bill twice Two different member service responses May have conflicts between Medicare and Medicaid networks MN Integrated SNP Features Integrated person centered care coordination, assessments and MOC Same enrollment requirements for both programs (State as TPA) One integrated enrollment form Same accretion and deletion dates for all Medicare and Medicaid services Coordinated member materials review with State, SNPs and RO One card and EOC, directories, materials,. One set of integrated notices Integrated QA, PIPs and QI Integrated coverage decisions and coverage flexibility for Medicare and Medicaid, waivers of 3 day hospital stays, in lieu of hospital days, etc. Integrated provider billing Integrated member services Integrated provider networks Typical SNPs vs. Integrated SNPs
MN Alternative Dual Demo Proposal • One of 15 Original Dual Demo states • Stakeholder involvement for refocusing dual programs over past 24 months • Stakeholder groups at State level and at each plan level required • Submitted proposal for both Capitated FAD and Original Demo • Withdrew Capitated FAD in June, 2012 with CMS understanding and support • Capitated FAD savings not viable due to 15 year history of integration • Many FAD features already similar to current MN programs • Much integration possible through SNP model • But State needs a role with Medicare, and Medicare needs to tweak SNP model to allow continued integrated
MN Alternative Alignment Demo • MSHO Seniors: State proposing alternative “Demonstration to Align Administrative Systems for Improvements in Beneficiary Experience” Builds on current SNP platform along with some FAD parameters • No new procurement/applications needed, builds on current D-SNPs • Current SNP and Medicaid financing and rates • Goals: • Improve SNP platform to align with and support State Payment and Delivery Reforms as developed through stakeholder efforts • Provide State a clearer joint role with CMS in Medicare SNP oversight • Preserve/enhance integrated administrative and operational features and reduce reliance on informal CMS Medicare SNP policy agreements which often change and threaten disintegration • Improve integrated D-SNP administrative efficiency and alignment for beneficiaries • Status: CMS Memorandum of Understanding (MOU) close to final, implement in 2013-2014
Proposed Demo Alignment Areas • Enrollments • Retain State TPA role, ensure facilitation of integrated enrollment forms and dates • Medicaid eligibility verification needed before Medicare enrollment is complete • Networks • Coordinate Medicare and Medicaid network adequacy standards • State involvement in exceptions process • Models of Care and Assessment • Assure continued integration of assessments (365 day issue) • Reduce duplication between MOCs and S&Ps • Member Materials • Retain integrated Evidence of Coverage, Summary of Benefits, member notices and communications, • Use new models from FAD where possible
Proposed Demo Alignment Areas • Quality Oversight • Test more targeted duals outcome measures (also working with NCQA on this) • Test alternative Stars Measures • HOS languages relevant to populations served • Consolidate CAHPs reporting with shared analytic data with state • Retain Integrated Benefit Determinations and Provider Billing • Clarify bid audit instructions • Premium Protection for Beneficiaries • Exploring mechanisms such as increasing in de-minimus premium levels (CMS objecting thus far) • Waive Part D co-pays as under FAD (no response from CMS on this yet) • Integrated Appeals and Grievances • Align State and CMS timelines (using FAD rules) • Simplify member materials
MN’s Alternative Demo: People with Disabilities 18-64 • Seeking separate MOU for dually eligible people with disabilities ages 18-64 • SNP model has not been financially viable in MN for this group • 5 SNPs for this population dropped out of Medicare due to bids generating premiums duals cannot pay, so seeking Medicare FFS demo option • Would include dual eligibles in both FFS and in Special Needs Basic Care (SNBC), a Medicaid managed care program that enrolls about half of the Medicaid disability population (45,000) • SNBC integrates behavioral health but LTSS remains FFS • Builds on current Medicaid State Plan Health Care Delivery Systems (HCDS), an innovative provider direct contracting option (Medicaid ACO type system) • HCDS organizations currently serve enrollees in both FFS and Medicaid MCOs including SNBC members • Goal is to incorporate Medicare into HCDS model • Feasibility currently under discussion with CMS
Payment and Delivery Reform: Integrated Care System Partnerships
MN Payment/Delivery Reform Initiatives • Health Care Home (HCH): Medicaid benefit provides additional payments to clinics and practitioners certified by MDH • Multi Payer Advanced Primary Care Practice (MAPCP) Demo: 8 state demo providing added Medicare payments to HCH for FFS patients including duals • Private Sector and Medicare ACOs: History of HMO/Provider ACO type subcontracting, also 3 Medicare Pioneer ACOs • Health Care Delivery System (HCDS): Primary/acute Medicaid ACO like delivery models operating in and outside of managed care • State Innovation Model (SIM): State’s CMS proposal accelerates adoption of ACO models (HCDS, Medicare ACOs, etc.) to improve care coordination, population health, patient experience and costs by building on the foundation of programs such as HCH/MAPCP • Dual Demo Integrated Care System Partnerships (ICSPs): SIM/HCDS aligned proposals for provider payment and delivery reforms within D-SNPs. • Combined Medicare and Medicaid provides incentives for provider level payment and delivery reforms stimulating subcontracting arrangements across all services. • Encourages involvement of long term care providers under shared pooled incentives. • Tied to quality and financial performance metrics
Payment/Delivery Reforms for MSHO Seniors • SNPs provide MSHO care coordination directly or through contracts with counties, Care Systems/Health Care Homes or community case management organizations. Unlike typical HCBS case management, care coordination models include clinical support for care coordinators to increase monitoring of chronic medical conditions. • SNPs and providers rely on integrated benefit determinations and the flexibility provided in Medicare Advantage to provide additional care coordination, waive 3 day hospital stays, provide in lieu of days, substitute services and support increased use of physician extenders in order to obtain these results. • Under MSHO, integrated financing has resulted in creative “Care System” (mini-ACO like) subcontracts for integrated service delivery and payment reforms across Medicare, Medicaid, primary acute and long term care with a range of arrangements such as: • Shared incentive pools or performance based payments with LTC providers • Combined Medicare and Medicaid care coordination PMPM payments • Combined Medicare and Medicaid primary care, Health Care Home and care coordination PMPM payments • Total cost of care sub-capitations or virtual sub-capitations with shared performance pools across all services • State goal is to increase the use of these payment and delivery reforms • Cooperation of Medicare SNPs and the Dual Demo are key to that goal.
Integrated Care System Partnerships • New 2013 contract provisions for SNP/MCOs participating in MSHO/MSC+/SNBC • Builds from current MCO/Provider “Care System” contracting arrangements (current providers may convert to ICSPs) • Combined Medicare and Medicaid financing provides incentives for provider level payment and delivery reforms stimulating new subcontracting arrangements and affiliations across services. • All models to incent improved health outcomes and choice of care setting • Seniors: Encourages involvement of long term care providers under shared pooled incentives or payment reform models • People with Disabilities: Encourages coordination of physical and behavioral health for people with disabilities in SNBC
Integrated Care System Partnerships • All proposals subject to State contract requirements for care coordination, quality metrics, financial performance measurement and reporting • Tied to a range of quality and financial performance metrics • Clinical workgroups developed quality measure options • Measures will differ between systems based on many factors: size, population served, setting of care, geographic area, etc. • ICSPs can propose alternative measures • Financial metrics proposed according to broad State parameters • SNP/MCO/Provider proposals due July 2013, review of proposals by State, provider contracts by October/13, implementation of new arrangements no later than January 2014.
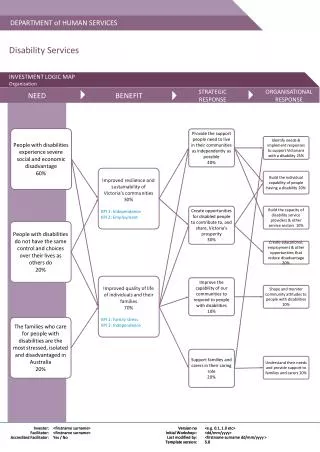
Revised Dual Demo Original Design Model : S pecial Needs Plan/Medicare Medicaid Integrated Care Organizations 8/13/2012 Virtual Care Systems MSC+ : CMS Medicare Contract and State Medicaid Contract Communication Tools Medicaid Payment to SNP and Payment to MCO/SNP coordinates Model 1 Medicare Primary and Acute Medicaid State Plan and Acute with Original Care LT SS M edicare SNP MMICO DEMO PLAN S PAC/NF Special Needs Plan Medicare and Medicaid Integrated Care Organizations LTSS Contract Requirements and Care Coordination Risk MMICO/Counties/ - Demo under Medicare Advantage Special Needs Plan Tribes/Community (SNP) platform and payment structures Organizations - Includes Medicare , Part D, current Medicaid State Chemical & plan and LTSS (seniors) starting 2013 - SNBC TBD for 2014 Phase 2 M en tal - MOU to outline State/CMS oversight roles HCH /Clinic Health Model 2: Integrated Care Model 3: Specialized ICSPs - CMS acknowledgement of State payment and Mental, Chemical and System Partnerships (ICSP) and/or HH delivery reform goals Physical Health DHS establishes criteria for model - “Rules for duals” supports features needed to - DHS establishes criteria for options for ICSPs including: integrated chemical, mental continue and improve integrated operational features - Primary care / payment reform s Acute and physical health care including quality and outcomes measurement and - Integrated care delivery Care system models for people with - TCOC accountability and options for integrated benefit determinations, provider billing SMI enrolled in SNBC under the risk/gain sharing arrangements and protection from premiums for enrollees demonstration -- Opportunities for - DHS issues RFP PAC/NF/LTSS/MH/CD providers - Requires partnership between - HCH Certification/Transition to HCH county, MMICO, primary care, - Enrollee choice of ICSP Market Incentives Acronyms chemical and mental health - Incentives to serve people across all CD - Chemical Dependency providers settings CMS=Centers for Medicare and Medicaid and Stimulation - Could also include non - dual - Standardized o utcome m easures FFS=fee for service SNBC members New ICSPs HCH=Health Care Home - Additional details TBD with - DHS Issues RFPs to stimulate HH=Health Home Chemical and Mental Health additional ICSPs ICSP=Integrated Care System Partnership and Continuing Care - Provider/MMICO Partnership LTSS=Long Term Services and Supports - Exploring Health Homes required for response MMICO=Medicare Medicaid Integrated Care Organization and/or HCH as part of model - DHS sets payment and risk/gain MSC+=Minnesota SeniorCare Plus - Standardized outcome options and parameters MSHO=Minnesota Senior Health Options measures Existing Care Systems NF= Nursing Facility - Dependent on viable Medicare - DHS evaluates current care systems PAC=Post Acute Care financing under demo for dual arrangements, those meeting or SNBC=Special Needs BasicCare eligibles with disabilities exceeding criteria would be SNP=Medicare Advantage Special Needs Plan - considered ICSPs SMI=Serious Mental Illness - Transition to HCH if not already HCH TCOC= Total Cost of Care - Standardized outcome measures
Complex Measurement Environment • Overlapping and unaligned measurement requirements from CMS and State levels for both plans and provider • CMS SNP and Part D requirements (STARS: HEDIS/CAHPs/HOS, S&Ps, MOC) often not relevant or applicable to people with dual status • State Medicaid requirements (HEDIS, CAHPs, Home and Community Based Services, EQRO, State Contract and Performance Withhold measures) • CMS Provider Measures: PQRS, CQMs, MDS, OASIS, ACOs • MN based provider performance measures (Minnesota Community Measurement, Health Care Homes, SQRMs, ACOs/HCDS, ICSPs) • Dual Demonstration Measures • Dual Demo Plan level measures and performance withholds • Dual Demo Provider level (ICSPs) measures • CMS Dual Demo Evaluation (over 100 measures being applied to FAD) • How can plans and providers best focus efforts on the small but important population of people with dual eligibility in the midst of these complex requirements?
Medicare HOS Medicaid HEDIS Measures Medicare HEDIS Measures Star Quality Ratings Other CMS Administrative Data Medicare CAHPS Survey SNP Structure and Process Measures SNP Model of Care Required Federal Reporting for Medicare-Medicaid SNPs
Health Plan Level Provider/Physician Group/Facility Level State HEDIS Statewide Quality Reporting and Measurement System (SQRMS) Minnesota Community Measurement Health Care Delivery System Measures Health Care Home Measures Contract Withholds State LTSS Medicaid CAHPS State Reporting Requirements
Measurement Challenges • Many current measures and accepted benchmarks are not appropriate for, or exclude old-old and younger disabled or those with multiple complex conditions • Recent progress (e.g. NQF MAPs) but we still lack sufficient consensus or experience with specific measures for these populations and many proposed measures are still in development/discussion phases • Members include many subpopulations with highly variable care trajectories, difficult to risk adjust let alone measure and assign benchmarks/expectations • Small numbers further complicate measurement • Difficult to define meaningful outcome measures for some highly variable domains of care (such as care coordination), but process measures are resource intensive and also may cause controversy (for STARS CMS wants outcome not process measures)
Measurement Challenges • Baseline and benchmark data may not exist, Medicare data still difficult to access, unclear data sources for some measures • Outside of HCBS survey measures of consumer satisfaction, attributing outcomes to any specific home and community based services is extremely problematic (i.e. Assisted Living, PCA, chore services, adult day care, home delivered meals, consumer directed options) • Utilization of consumer directed options not as good a measure for seniors, fewer use it due to percieved management burdens • Multiple levels of providers with overlapping responsibility make it difficult to assign accountability (PCP, Specialists, Rehab, S/NFs, Residential vs SNP level?)
Minnesota’s Proposed ICSP Measures Measure Identification and Development Process • RFPI to solicit public input to best practices in mid January • January 28, 2013: Policy Symposium to discuss best practices • Mid February: RFPI comments due • Clinical workgroup of SNP Medical Directors and QA staff • Alignment discussions with local and national measurement experts (NCQA, Health Department, Minnesota Community Measurement, Stratis QIO, Board on Aging, etc) • Discussion with Provider Care Systems • Discussion with Stakeholders groups Proposed ICSP Measures for all populations/settings • Hospital Utilization • Plan All Cause Readmissions • Potentially Preventable Readmissions • Ambulatory Care Sensitive Conditions Admission Rates • Ambulatory Care and ED Visits Especially for MSHO Institutional Members • Use of Antipsychotics for People with Dementia • Falls with Fx • Pressure Ulcers • S&P: Evidence of POLST with person specific goals for residents with 90 day+ stays • S&P: Follow Triage Protocol prior to sending to ED or inpatient stay
Minnesota’s Proposed ICSP Measures Especially for MSHO Community Frail Elderly (average age 80+) • Flu Shots/Pneumococcal Vaccination Status • Use of High Risk Medication in the Elderly • Annual Monitoring of Patients on Persistent Meds • Medication Reconciliation Post Discharge • Care of Older Adults • S&P: Reduced Risk of Falls/Falls Screenings Fall Risk Management • Best Practice Incentive S&P: Care Transitions (TBD) • *Best Practice Incentive S&P: Evidence of Functional Assessment Response by PCP • *Best Practice Incentive S&P: Evidence of ongoing PCP/Care Coordinator Communication • *Best Practice Incentive S&P: Evidence of Integrated Care Plan for Community Members * Potential collaboration with NCQA Especially for People with Disabilities 18-64 in SNBC (all settings) • Anti-Depressant Medication Management • Follow Up after Hospitalization related to Mental Illness (and Substance Abuse) • Adult Access to Preventive/Ambulatory Health Services • Basic Preventive Screenings (Cholesterol, Colorectal Cancer, Breast Cancer, Flu Shots) • Screenings for Clinical Depression and Follow Up • Pressure Ulcers • S&P: Evidence of Behavioral and Physical Health Integration, Communications and Care Planning (TBD)
Summing It Up • National effort for improved alignment and delivery system integration of Medicare and Medicaid for people with dual status, CMS is implementing new initiatives in many states, MN in the lead. • MSHO will return to demo status • Not much will visibly change from current program, but program will support new delivery system mechanisms and give the State role in SNP oversight • State pursuing a different demonstration for people with disabilities based on HCDS model, early in process but stay tuned • SIM will provide framework for new payment and delivery reform efforts in MN • MSHO/SNBC aligning with new delivery systems through formation of new ICSPs and HCDS • ICSPs expected to further integrate primary care, behavioral health and LTSS care coordination mechanisms • ICSPs will link clinical and financial performance • Measurement will be challenging and will have to evolve over time!
Minnesota Medicare Medicaid Integrated Programs and Dual Demo Contact Information:Pamela Parker, MPA, Manager pam.parker@state.mn.us651-431-2512 Sue Kvendru, Seniors Managed Care CoordinatorSue.Kvendru@state.mn.us651-431-2517Deb Maruska, Project Manager, Dual Demo/Disability Managed CareDeb.maruska@state.mn.us651-431-2516 Dual Demo Stakeholders Website:www.dhs.state.mn.us/DualDemoDisability Managed Care Stakeholders Groupwww.dhs.state.mn.us/SNBC
MSHO SNPs/MSC+ MCOs • Blue Plus • Health Partners • Itasca Medical Care • Medica • Metropolitan Health Plan • Prime West • South Country Health Alliance • UCare Minnesota * All plans offer both MSHO SNP and MSC+ Medicaid plans
SNBC SNPs/MCOs • Medica • Metropolitan Health Plan * • Prime West* • South Country Health Alliance* • UCare Minnesota *Offers Medicare Dual Eligible SNP for SNBC