Download
1 / 1
10 likes | 106 Views
This study evaluates the impact of "Term BMI" instead of pre-pregnancy BMI on cesarean section risk, estimated blood loss, and neonatal weight. Findings indicate a significant association between increasing BMI and delivery outcomes. The research emphasizes the importance of assessing obesity risks accurately. Using Term BMI at delivery provides a more precise evaluation of delivery complications. This retrospective study offers insights into delivery risk factors based on BMI categories.

E N D
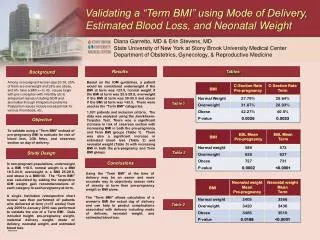
Validating a “Term BMI” using Mode of Delivery, Estimated Blood Loss, and Neonatal Weight Diana Garretto, MD & Erin Stevens, MD State University of New York at Stony Brook University Medical Center Department of Obstetrics, Gynecology, & Reproductive Medicine Results Tables Background Based on the IOM guidelines, a patient would be considered underweight if the BMI at term was <23.5, normal weight if the BMI at term was 23.5-29.9, overweight if the BMI at term was 30-33.5 and obese if the BMI at term was >33.5. These were used as the “Term BMI” categories. 1,031 patients met inclusion criteria. The data was analyzed using the Jonckheere-Terpstra Test. There was a significant increase in risk of cesarean section with increasing BMI in both the pre-pregnancy and Term BMI groups (Table 1). There was also a significant increase in estimated blood loss (Table 2) and neonatal weight (Table 3) with increasing BMI in both the pre-pregnancy and Term BMI groups. Among non-pregnant women age 20-39, 25% of them are overweight and 28% are obese, and 6% have a BMI >= to 40. Issues begin with pre-conception with infertility etc to antepartum issues including GDM and anomalies through intrapartum problems. Postpartum issues include increased risk for venous thrombosis, etc. Table 1 Objective To validate using a “Term BMI” instead of pre-pregnancy BMI to evaluate for risk of blood loss, LGA fetus, and cesarean section on day of delivery. Table 2 Study Design Conclusions In non-pregnant populations, underweight is a BMI <18.5, normal weight is a BMI 18.5-24.9, overweight is a BMI 25-29.9, and obese is a BMI>30. The “Term BMI” was calculated by adding the respective IOM weight gain recommendations of each category to each pregnancy at term. A single institution retrospective chart review was then performed of patients who delivered at term (>=37 weeks) from July 2009 to January 2010 was performed to validate the use of a Term BMI. Data included height, pre-pregnancy weight, maternal delivery weight, mode of delivery, neonatal weight, and estimated blood loss. Using the “Term BMI” at the time of delivery may be an easier and more accurate way to objectively assess risks of obesity at term than pre-pregnancy weight or BMI alone. The “Term BMI” allows calculation of a woman’s BMI the actual day of delivery and can help to predict complications associated with delivery including mode of delivery, neonatal weight, and estimated blood loss. . Table 3