Download
1 / 13
130 likes | 371 Views
Hematology Case 2: Woman with Dyspnea and Fatigue Submission date : Monday, June 16, 2014. Tanni- Presenter Victor- Team Leader Asma- Editor Sarwar- Timekeeper. Hematology Case 2 Overview. History Physical Examination Lab Investigations: results and interpretation

E N D
Hematology Case 2: Woman with Dyspnea and Fatigue Submission date: Monday, June 16, 2014 Tanni- Presenter Victor- Team Leader Asma- Editor Sarwar- Timekeeper
Hematology Case 2Overview • History • Physical Examination • Lab Investigations: results and interpretation • Assessment: DDx and most likely Dx • Management • Prognosis and Patient education
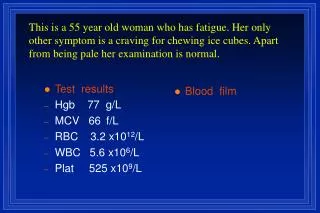
History 67 year old female with shortness of breath on exertion, easy fatigability, and lack of energy for the past 2 to 3 months. Denies GI, or vaginal bleeding. Denies hemoptysis. Described a good diet but variable appetite.
Additional Relevant History Questions • What is her PMHx? • What is her family history? • Is she currently on any medications (OTCs, Herbal included)? • What is her alcohol intake? Smoker? • Is there any chest pain? • Any symptoms of jaundice or dark coloured urine? • Any sudden weight loss? • Any recent trauma?
Physical Exam Skin pallor noted. The rest of the physical examination is unremarkable.
Laboratory Investigations RBC 3.72 x 1012/L Hgb 58 g/L Hct 0.208 MCV 56.1 fL MCHC 285 g/L RDW 0.204 WBC 5.8 x 109/L Neutrophils 82 % Lymphocytes 13 % Monocytes 1 % Eosinophils 4 % Basophils 0 % Platelets 387 x 109/L serum ferritin <10 µg/L serum iron 4.5 µmol/L TIBC 127.5 µmol/L transferrin saturation 4 % Fecal occult blood negative Blood smear analysis RBC morphology 1+ anisocytosis2+ elliptocytes and target cells 2+ hypochromasia2+ microcytosis WBC morphology normal Platelet morphology normal
Interpretation of Lab Results(key findings) • Low RBC , Hgb and Hct levels ( RBC < 4.0 x 1012/L , Hgb < 120 g/L, Hct < 37%) => Anemia • MCV of 56.1 fl => Microcytosis (<80 fl) • MCHC of 285 g/L => Hypochromia (<327 g/L) • So far, this is Microcytic Hypochromic Anemia • Low ferritin ( < 45 µg/L), High TIBC ( > 66 µmol/L) and RDW (> 15%)=> Iron Deficiency • Transferrin saturation of 4% doesn’t fit the pattern of Iron Deficiency (should be increased above 12-45% for females • High level of neutrophils (> 73%), low lymphocyte level (< 20%) and low monocyte level (< 2%) are non-specific findings at this stage
Differential Diagnosis with brief explanation of rationale • Microcytic Hypochromic Anemia (Iron Deficiency Anemia) • Anemia of Chronic Disease • Renal failure • Liver Disease • Neoplasia carcinoma • Leukemia
Most Likely Diagnosiswith brief explanation of rationale Iron Deficiency anemia It is a type of Microcytic Hypochromic Anemia. Rationale • Microcytosis, hypochromasia. • Presence of the target cells • Absence of any blood loss and negative FOBT • Low serum Iron, Low ferritin and high iron binding capacity. • Absence of inflammation or any comorbid conditions.
Pathophysiology Categories • iron deficient • impaired Hb production Etiologies • GI blood loss • Menstrual blood loss • Decreased iron absorption • Hemolysis (less common)
Management Non Pharmacological Choices: • Dietary Iron -foods rich in heme iron • Promoter: Vitamin C • Inhibitor: Tea, Coffee Pharmacological Choices: • oral iron supplements (ferrous gluconate, ferrous sulfate, ferrous fumarate) • Paranteral Iron
Prognosis/Patient Education Iron Deficiency Anemia has a good prognosis if treated properly with iron supplementation. Patient Education: iron-deficiency is when there is an insufficient amount of iron in the body. Iron is required to bind oxygen to hemoglobin which carries it to the body tissues. Signs and Symptoms: Dyspnea, fatigue, pale coloration of the skin. Prevention: Prevented by proper intake of iron in the diet. Diet should include meat, green leafy vegetables, enriches breads/grains, fruits. Iron absorption is increased when taken with Vitamin C and decreased when taken with caffeinated drinks.
References 1) Beers M., Berkow R., “Overview of Anemia”, The Merck Manual of Diagnosis and Therapy, 17th Ed., New Jersey, pp 561 2) Harper J., “Iron Deficiency Anemia”, Medscape, Retrieved on June 11, 2014, http://emedicine.medscape.com/article/202333-overview 3) “Causes and Diagnosis of Iron Deficiency Anemia in the Adult”, UpToDate, Retrieved on June 11, 2014, http://www.uptodate.com/contents/treatment-of-the-adult-with-iron-deficiency-anemia 4) Lee M ., “Hematology Red and White Blood Cell Tests”, Basic Skills in Interpreting Laboratory Data, 5th Edition, Ch. 15, pp 353-369