Download
1 / 22
220 likes | 402 Views
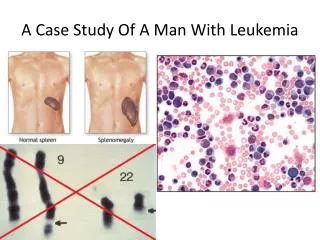
A Case of a man with relentless headache. Calma * Capili * Dagang * Dayrit. General Data. FV 49/M Married, Roman Catholic, from Canlubang Laguna Admitted to the PGH ER last April 2, 2010. Chief Complaint. Headache for 5 months. History of Present Illness.

E N D
A Case of a man with relentless headache Calma * Capili * Dagang * Dayrit
General Data FV 49/M Married, Roman Catholic, from Canlubang Laguna Admitted to the PGH ER last April 2, 2010
Chief Complaint Headache for 5 months
Review of Systems (-) abdominal pain (+) 3 P’s (-) bowel complaints (-) seizures (-) loss of consciousness (-) edema • (+) weight loss (25% in 5 months) • (-) anorexia • (-) fever • (-) cough, colds • (-) difficulty of breathing • (-) chest pain
Past Medical History (+) HPN – since 2000, UBP 160/100, HBP 180/120, (-) maintenance medications (+) DM – since 2003, (-) maintenance medications (-) PTB, BA, allergies, history or trauma, previous surgeries
Family Medical History (+) HPN – father (-) DM, PTB, BA, CA
Personal Social History Truck driver, married with 6 children Non-smoker, occasional alcoholic beverage drinker, (-) illicit drug use
Physical Examination BP 130/90 HR 90 RR 20 PC, AS, (-) CLAD, (-) ANM ECE, CBS, (-)crackles/wheezes (-) heaves/thrills, DHS, NRRR, AB 5th ICS LAAL, (-) murmurs Abdomen flat, NABS, soft, non-tender FEP, PNB, (-) clubbing, (-) edema
Neurologic Examination GCS 15, alert, awake, oriented to 3 spheres Cranial Nerves
Neurologic Examination Motor Good muscle bulk, (-) spasticity, (-) flaccidity 5/5 5/5 5/5 5/5 Sensory 100% 100% 100% 100%
Neurologic Examination DTRs ++ ++ ++ ++ ++ ++ Cerbellars: (-) dysmetria, (-) dystiadochokinesia Meningeals: (-) nuchal rigidity, (-) Kernig’s, (-) Brudzinski Autonomic
Cranial CT Scan (+) contrast enhancing tumor, ill defined involving sellar-supresellar, sphenoidal areas
Cranial CT Scan Insert plates here
Cranial MRI with GAD (+) sellar-supresellar mass occupying the sphenoid sinus as well (+) encasing B cavernous sinus with invasion of clivus Impression: Chordoma vs. Invasive Pituitary Adenoma
Cranial MRI with GAD Insert plates here
Other Laboratory Exams CBC: 4/2: Hgb 103 Hct 0.309 WBC 7.1 N 0.652 L 0.276 Plt 331 PT/PTT: 4/2: 11.0/12.2/0.89/1.17; 32.6/37.3 4/5:FT4 8.4 (N 11-24 pmol/L), TSH 0.8 (N 0.3-3.8 mIU/L), Cortisol25 (N 138-690 nmol/L), PRL 3,041.9 (80-430mIU/L)
Course in the ER In the ER, pt managed primarily by NSS, co-managed by ORL, Ophtha, and Endo Pt GCS 15 while in the ER, no motor or sensory deficits. Pt on the following medications: Mannitol 75 cc IV Q8 Q6, Celecoxib 200 mg/cap Q12, Tramadol 50 mg/tab TID Tramadol 50 mg IV Q8, Ketorolac drip (30 mg in 250cc D5W x 24h), Dexamethasone 5 mg/IV Q6
Course in the ER ORL: A> hearing loss etiology to be determined. Plan for PTA-ST and for transsphenoidal biopsy/GA once admitted Ophtha: A> LR palsy probably secondary to malignancy. Refraction done. Plan for visual perimetry.
Course in the ER Endo: A> Consider secondary hypogonadism, secondary hypothyroidism, secondary hypoadrenalism secondary to suprasellar mass with mass effect. Hyperglycemia probably secondary to DM vs. steroid induced vs. combination. Hyponatremia secondary to SIADH due to tumor, secondary hypothyroidism, secondary to AI, secondary to mannitol use, orsecondary to hyperglycemia. Pt started on Levothyroxine 100 mcg/tab 30 min before breakfast, HN 20-0-10 SQ pre-melas, HR 8-8-8 SQ pre-meals, defer for CBG < 70mg/dL.