PCOS
PCOS FOR MEDICAL STUDENT PRESENTATION


PCOS
E N D
Presentation Transcript
PCOS(Poly Cystic Ovarian Syndrome) DR. SAGAR D DHERANGE MS OBGYN-A
Irving F. Stein, Sr., Michael L. Leventhal Stein Leventhal Syndrome (1935)
WHY TO STUDY • HIGH PREVALANCE RATE • COMMONEST ENDOCRINE DISORDER DURING REPRODUCTIVE AGE • COMMONEST CAUSE OF INFERTILITY • COMMONEST TREATABLE CAUSE OF INFERTILITY , IF DIAGNOSED • COMMONEST COMPLAINT IN UNMARRIED PATIENTS OF GYNAECOLOGY • OFTEN ASSOCIATED WITH OBESITY, HIRSUITISM, INFERTILITY , ENDOCRINOPATHY
PREVALANCE • (AS PER WHO, 7 February 2025) • Polycystic ovary syndrome (PCOS) affects an estimated 6–13% of reproductive-aged women. • Up to 70% of affected women remain undiagnosed worldwide. • PCOS is the commonest cause of anovulation and a leading cause of infertility.
PREVALANCE IN INDIA • prevalence of PCOS from 2010 to 2021- • close to 10% using Rotterdam's criteria and AES criteria • while it was 5.8% using the NIH criteria. (1) • Amongst infertile women, about 20% infertility is attributed to anovulation caused by PCOS.(2)
DEFINATION It is a heterogeneous condition characterized by menstrual irregularity, hyperandrogenism, obesity and polycystic ovaries on ultrasound.(3)
AETIOLOGY • EXACT CAUSE- UNKNOWN • Risk FACTORS • change in lifestyle, diet and stress • Genetic factors - CYP21 gene mutation • familial factors - X-linked dominant mode of inheritance • environment factors- in the utero or in early adolescent life,
Pathological events • 1) HPO - abnormality • 2) Hyperandrogenism • 3) Insulin Resistance • 4) Anovulation • 5) Obesity
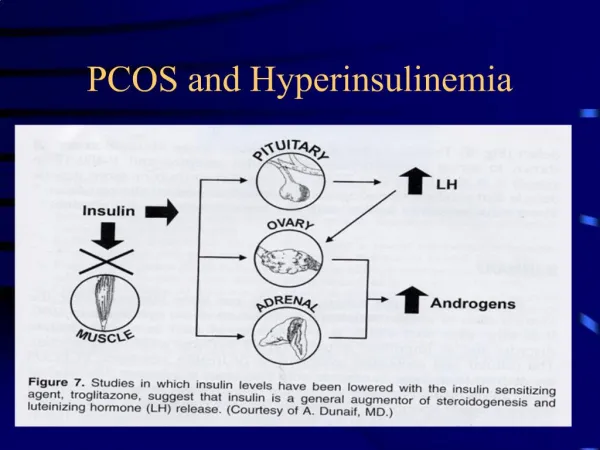
MAIN CULPRIT • Insulin resistance • Reduced insulin reception activity peripherally insulin resistance • Hyperandrogen • Enhanced serine phosphorylation unification activity in the ovary
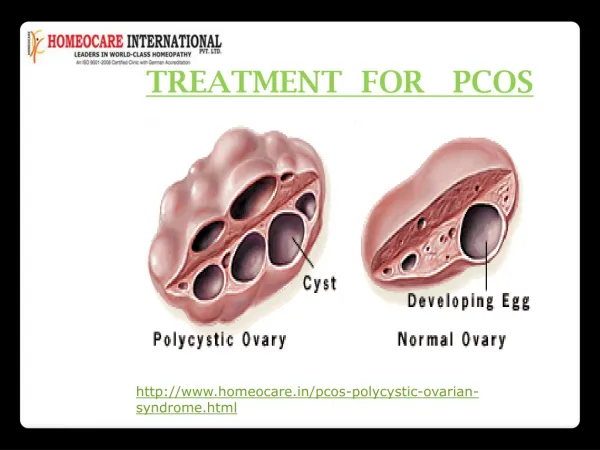
Diagnostic criteria ESHARE (Rotterdam) 2003 • Irregular menses • Hyper Androgenism • Polycystic appearance on USG
Diagnostic criteria ESHARE (Rotterdam) 2003 • Any 2 of following 3 to be present • 1) Oligo or Anovulation • 2) Clinical or biochemical hyperandrogenism • 3) Polycystic Ovaries on Ultrasound • 12 or more follicles • Each follicle 2-9 mm in diameter • Necklace pattern of follicles • Ovarian volume > 10 cm³
Rotterdam Criteria 15 August 2023 • any 2 of the following 3 criteria • 1. Anovulation presented as amenorrhea or oligomenorrhea • 2. Hyperandrogenemia (excess of androgens/testosterone) or hyperandrogenism presented as hirsutism • 3. PCOM - Polycystic Ovarian Morphology on USG meaning volume of each ovary more than 10 ml and /or number of follicles greater than 20 (size 2-9mm).
Clinical features • 1) Menstrual Abnormality- oligomenorrhoea, Amenorrhoea or DUB • 2) Obesity • 3) Hirsuitism • 4) Acne, Alopecia • 5) Viralism • 6) Acanthosisnigricans- Thickening & pigmentation of skin at nape of neck, inner thighs, groins, axilla due to insulin resistance
HAIR-AN syndrome • 1) Hyper Androgenism. • 2) Insulin Resistance • 3) AcanthosisNigricans.
Endocrine Abnormalities 1) Elevated LH 2) Normal FSH 3) Elevated LH: FSH Ratio (>3:1) 4) Elevated Androgen 5) Low SHBG (Sex hormone Binding Globulin) 6) Mildly elevated prolactin 7) Elevated fasting insulin 8) Abnormal glucose tolerence test 9) Dyslipidaemia
Complications • 1) Obesity • 2) Dyslipidaemia • 3) Diabetes mellitus • 4) Coronary heart disease • 5) Endometrial & Breast cancer
WHAT INVESTIGATION HAS TO BE DONE…? • BODY MASS INDEX • SR INSULIN • SR FSH • SR LH • SR TESTOSTERONE • SR SHBG • SR PROLACTIN • THYROID FUNCTION TEST • HBA1C • LIPID PROFILE • SR AMH
Management • 1) Weight Reduction • INTERMITTENT FASTING • EXERCISE
2) Combined OCP • Desogesterol + Ethinyl estradiol- Tab Femilon • Cyproterone Acetate + Ethinyl estradiol Tab Krimson • Drospirenone + Ethinyl estradiol Tab Dronis
3) Insulin sensitizers • Metformin 500 mg OD - Tab Glycomate • Myoinositol & D ChiroInositol Vit D3 - Tab OvacetForte • Berberin Extract Myoinositol & D Chiro Inositol Vit D3 Tab Beritol
Treatment for Hirsutism • Anti Androgens- Cyproterone • Laser techniques
Treatment for infertility • Ovulation induction – letrozole, clomiphene citrate
Surgery – Laproscopic Ovarian Drilling • Bariatric Surgery
References • BharaliMD, Rajendran R, Goswami J, Singal K, Rajendran V. Prevalence of Polycystic Ovarian Syndrome in India: A Systematic Review and Meta-Analysis. Cureus. 2022 Dec 9;14(12):e32351. doi: 10.7759/cureus.32351. PMID: 36628015; PMCID: PMC9826643. • Howkins & bourne, Shaws Textbook of Gynaecology , Elsevier Publication ,16th Edition , Page No 431 • Lakshmi sheshadri, Essentials of Gynaecology, second edition, Wolters Kluwer (India) , Page No 268 • Sagar Dherange, Smita Chodankar, A Concise Textbook Of Obstetrics & Gynaecology, Walnut Publication October 2024, Page No 470