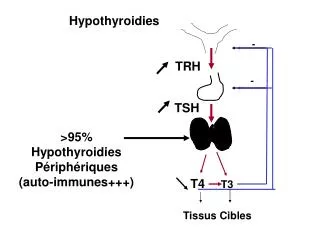
T4 T3
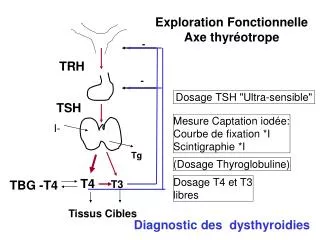
Exploration Fonctionnelle Axe thyréotrope. -. TRH. -. Dosage TSH "Ultra-sensible". TSH. Mesure Captation iodée: Courbe de fixation *I Scintigraphie *I. I-. Tg. (Dosage Thyroglobuline). T4 T3. Dosage T4 et T3 libres. TBG -T4. Tissus Cibles. Diagnostic des dysthyroidies.

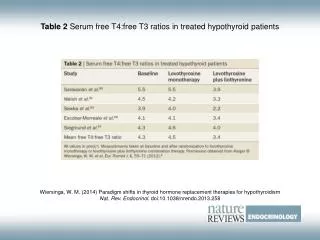
T4 T3
E N D
Presentation Transcript
Exploration Fonctionnelle Axe thyréotrope - TRH - Dosage TSH "Ultra-sensible" TSH Mesure Captation iodée: Courbe de fixation *I Scintigraphie *I I- Tg (Dosage Thyroglobuline) T4T3 Dosage T4 et T3 libres TBG -T4 Tissus Cibles Diagnostic des dysthyroidies
Exploration Morphologique Thyroidienne Oeil et Mains Echographie TDM (Sans Injection) (IRM) Diagnostic des Goitres et Nodules
Exploration Immunologique Anticorps Thyréostimulants (TRAK) Anticorps Anti-Thyropéroxydase (TPO) Anticorps Anti-Thyroglobuline Diagnostic des Thyroidites auto-immunes
Exploration cytologique et Histologique Cytoponction (aspiration) à l'aiguille Fine Analyse extemporanée pièce d'exerèse Analyse Histologique pièce d'exerèse
Exploration cellules C CALCITONINE à l'état basal +/- Pentagastrine Diagnostic du CANCER MEDULLAIRE
Thyrotoxicoses périphériques - TRH - TSH I- Tg T4T3 TBG -T4 Tissus Cibles
0,01 0,01 N N N TSH (mUI/l) T4 libre (pmol/l) T3 libre (pmol/l) 23 5 Euthyroidie Thyrotoxicose « infra-clinique » Thyrotoxicose
0,01 0,01 N N N TSH (mUI/l) T4 libre (pmol/l) T3 libre (pmol/l) 23 5 5 Euthyroidie Thyrotoxicose à T3 Thyrotoxicose à T4
TSH mUI/l Hypothyroidies Périphériques Hyperthyroidies Centrales 4 Euthyroidie Insuffisance Thyréotrope 0, 1 0, O1 Thyrotoxicose périphériques 0 9 23 T4 libre pmol/l
Suspicion clinique de Thyrotoxicose TSH <0,01uUI/ml N Pas de Thyrotoxicose périphérique Si certitude clinique de thyrotoxicose T4 libre
TSH <0,01uUI/ml T4 libre Insuffisance thyréotrope Thyrotoxicose N T3 libre « Syndrôme de Basse T3 » « Thyrotoxicose à T3 » N « Thyrotoxicose infra-clinique »
Thyréocyte Ultra-simplifié Pôle basal (capillaire) Pôle Apical (colloïde) I- TG TPO TSH T 4 T3 TG
Thyrotoxicose par Hyperthyroidie I- Ac Anti RTSH Basedow Mutations RTSH -Nodule toxique -Hyperthyroidie non auto-immune TSH dépendante Adénome thyréotrope Résistance hypophysaire hormones thyroidiennes TG TPO T 4 T3 TG
Thyrotoxicose par Hyperthyroidie Basedow+++ Femme/homme 4/1 Goître +/- orbitopathie Ac Anti RTSH Ac anti TPO évolution par poussées Hyperthyroidie familiale non auto-immune TSH dépendante Scintigraphie Iode 123 ou Tec 99
Thyrotoxicose par Hyperthyroidie Nodule toxique
Thyrotoxicose par Hyperthyroidie Surcharge iodée Amiodarone Produits de contraste Polyvidone iodée I- TG TPO T 4 T3 TG
Thyrotoxicose par Hyperthyroidie Surcharge iodée Iodémie Scintigraphie Iode 123 ou Tec 99
Thyrotoxicose par Destruction vésiculaire Thyroidites (phase initiale) -sub-aigüe -silencieuse (post-partum) -interféron -amiodarone TG TPO TG T 4 T3
Thyrotoxicose par Intoxication T4 (Levothyroxine) Iatrogène Traitement freinateur ou substitutif mal conduit Thyrotoxicose factice I- TG TPO T 4 T3 TG
Thyrotoxicose par Intoxication Thyroglobuline indétectable
Scintigraphie /Thyrotoxicose Basedow Hyperthyroidie familiale Hyperthyroidies TSH dépendantes Nodule Toxique GMultinodulaire toxique Thyroidites sub-aigüe , silencieuse, interféron amiodarone Tx par surcharge iodée Thyrotoxicose factice
Diagnostic étiologique d’une thyrotoxicose démontrée Goitre et Orbitopathie Oui Scintigraphie Basedow Fixation bilatérale Fixation élective 1 ou plusieurs nodules Fixation Très faible ou nulle Contexte de thyroidite? Iodémie Tg AcRTSH + ou AcTPO+ Oui Non Nodule toxique Goitre Multinodulaire Toxique Basedow Thyroidite/destruction Surcharge iodée Factice Basedow Hyperthyroidie familiale auto-immune
Traitement Thyrotoxicoses Antithyroidiens de Synthèse Iode 131 I- TG Perchlorate de K TPO TSH T 4 T3 PTU Propranolol + Chirurgie Tissus Cibles
Antithyroidiens de Synthèse Carbimazole (Néomercazole) Dose « bloquante » 40mg/j. Entretien 2,5 à 10 mg/j Propylthiouracile (PTU)db 400 mg/j, de 25 à 100 Effets indésirables majeurs : agranulocytose hépatites Effets indésirables mineurs: allergie cutanée
Iode 131 -Dose calculée en fonction captation -effet différé (qques mois) -à long terme: risque d ’hypothyroidie -pas de risque cancérigène démontré -risque tératogène supposé
Chirurgie thyroidienne Morbidité faible (2%) si chirurgien très entraîné -paralysie récurrentielle -hypoparathyroidie Lobo-isthmectomie (nodule toxique) Thyroidectomie sub-totale ou totale (Basedow)
Indications Basedow ATS 18 mois -soit NMZ dose bloquante, puis NMZ+LT4 substitutive -soit NMZ dose bloquante, puis NMZ dose entretien NFS++ en cas de fièvre (et 2/mois pdt 3 mois) Si récidive (ou après ATS 1 mois si très gros goître) Traitement radical -Chirurgie -Iode 131
Indications Nodule toxique ATS 1 mois (pour euthyroidie) Puis chirurgie ou Iode 131 si contre-indication chirurgie Thyroidite avec destruction vésiculaire propranolol (corticoides pour Thyroidite amiodarone) Surcharge iodée ATS+/-perchlorate; propranolol