Download

1 / 95
950 likes | 1.34k Views
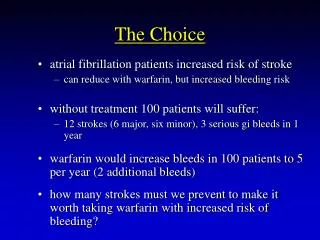
PANELISTS. Optimizing the choice in oral contraception. Dr Asha Bhatt Dr Dipti Patel Dr Bharat Rangani Dr Tejal Shah Dr Pooja Nadkarni. Case 1. A newly married girl comes to you for information about contraception.

E N D
PANELISTS Optimizing the choice in oral contraception Dr Asha Bhatt Dr Dipti Patel Dr Bharat Rangani Dr Tejal Shah Dr PoojaNadkarni
Case 1 • A newly married girl comes to you for information about contraception. • How would you approach this client in terms of contraception counselling & choice?
The Patient Interview:The Clinician’s Priorities • Recognize the patient’s goals for control of fertility • Identify the patient’s health risks that result in some methods being preferred over others WHO CATEGORY 4 • Determine the patient’s ability to consistently and correctly use the preferred method
Teaching Patients About Contraceptive Efficacy • Why efficacy depends on correct and consistent use • Why methods fail, even with proper use • Why long-term methods tend to have lower failure rates • Why using two methods simultaneously is more effective than using one alone • Why emergency contraception is a last chance to prevent pregnancy
What are the usual barriers to consistent and correct use of a contraceptive method?
Patient Barriers to Consistent and Correct Use of a Contraceptive Method • Experience with the method • Fears and misunderstandings • Ability to remember and use the method • Tolerance of side effects • Cultural, social, or moral concerns • Partner (or parental) objections
Principles of Effective Counseling • Listen actively • Assume nothing • Objective listening offers a common ground • Your patient may have more ways to solve her problems than you will • Believe that your patient knows what she wants • Respect your patient’s right to privacy Hatcher R, et al, eds. Contraceptive Technology. 18th rev ed. 2004.
Education Tools and Reminder Devices • Patient information handouts- • Correcting misperceptions • Non contraceptive health benefits • Daily alarm on a computer, personal digital assistant (PDA), or cell phone • Encourage her to call if she has questions or concerns
Myths and Misconceptions About Oral Contraceptives • Cause cancer • Cause blood clots • Are associated with weight gain • Should not be taken by women over the age of 35 • Disrupt an existing pregnancy if taken inadverently. • Makes woman infertile • Changes sexual behaviour • Build up in a woman’s body. Women need a “rest” from taking cocs.
No statistical difference in weight gain (0.5 kg) between users of oral contraceptives (30 g EE) and nonusers Weight Gain and Oral Contraceptives: Controlled Studies Do Not Show Link Weight gain (5 lb) in ~ 25% of women; no significant difference between the placebo group and the users of oral contraceptive ( 50 g ethinyl estradiol [EE]) Placebo-controlled double-blind crossover (N=380) Goldzieher et al., 1971 Prospective, randomized (N=49) Reubinoff et al., 1995 No association between combination oral contraceptives and weight gain Systematic review of randomized controlled trials Gallo et al., 2006 Goldzieher JW, et al. FertilSteril. 1971;22:609-623; Reubinoff BE, et al. FertilSteril. 1995;63:51 Gallo MF, et al. Cochrane Database Syst Rev. 2006;(1):CD003987.
30 µg EE/3 mg DRSP 20 µg EE/3 mg DRSP 15 µg EE/3 mg DRSP 30 µg EE/0.15 mg LNG Drospirenone Has Neutral Effects on Weight 1.0 0.5 0 -0.5 Mean Change in Body Weight (kg) -1.0 -1.5 -2.0 3 6 7 Month EE = ethinyl estradiol DRSP = drospirenone LNG = levonorgestrel Oelkers W, et al. J Clin Endocrinol Metab. 1995;80:1816-1821.
Risks of Oral Contraceptives:Nonfatal Venous Thromboembolism Estimated Average Risk/ 100,000 Women/Year Non-Oral Contraceptive Users Oral Contraceptive Users Pregnant Women Food and Drug Administration. FDA Talk Paper. Nov. 24, 1995.
Oral Contraceptives and the Risk of Breast Cancer • Results of a large epidemiologic study suggest that oral contraceptives do not cause breast cancer • Breast cancer risk in women who have not taken oral contraceptives for ≥10 years is the same as those who have never used them • There is a slightly increased risk of diagnosisin current users of oral contraceptives and in those who stopped taking them ≤10 years ago • Tumors are more likely to be localized in oral contraceptive users than in nonusers Collaborative Group on Hormonal Factors in Breast Cancer. Lancet. 1996;347:1713-1727; Collaborative Group on Hormonal Factors in Breast Cancer. Contraception. 1996;54:1S-106S.
Noncontraceptive Benefits of Oral Contraceptives • Improvement of cycle-related conditions: • Acne • Irregular menstrual cycles • Dysmenorrhea • Menorrhagia • Anemia • Functional ovarian cysts • Reduction in cancer of certain organs: • Ovary • Endometrium • Colon and rectum Wallach M, et al., eds. Modern Oral Contraception: Updates from The Contraception Report. Emron, 2000.
Studies Show Oral Contraceptives Reduce the Risk of Ovarian Cancer Hildreth et al., 1981 Rosenberg et al., 1982 La Vecchia et al., 1984 Tzonou et al., 1984 Booth et al., 1989 Hartge et al., 1989 WHO, 1989 Wu et al., 1988 Prazzini et al., 1991 Newhouse et al., 1977 Casagrande et al., 1979 Cramer et al., 1982 Willet et al., 1981 Weiss, 1981 Risch et al., 1983 CASH, 1987 Harlow et al., 1988 Shu et al., 1989 Walnut Creek, 1981 Vessey et al., 1987 Beral et al., 1988 Summary of relative risk with ever-use of an oral contraceptive: 0.64 (95% CI, 0.57-0.73) Hospital-Based Case-Control Study Community-Based Case-Control Study Cohort Study 0.5 1.0 1.5 2.0 2.5 3.0 3.5 0.0 Relative Risk Hankinson SE, et al. Obstet Gynecol. 1991;80:708-714.
Studies Show Oral Contraceptives Reduce the Risk of Endometrial Cancer Horwitz et al., 1979 Weiss et al., 1980 Kaufman et al., 1980 Kelsey et al., 1982 Hulka et al., 1982 Henderson et al., 1983 La Vecchia et al., 1986 Pettersson et al., 1986 CASH, 1987 Koumantaki et al., 1989 WHO, 1991 Brinton et al., 1983 Jick et al., 1993 Ramcharan et al., 1981 Trapido, 1983 Beral et al., 1988 Case Control Cohort 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 Relative Risk Adapted from Grimes DA, Economy KE. Am JObstet Gynecol. 1995;172:227-235.
Oral Contraceptives and Hip Fractures:Possible Risk Reduction Odds Ratio Over 40 Control Under 30 30-39 Age (Y) at First Oral Contraceptive Use Michaelsson K, et al. Lancet. 1999;353:1481-1484.
Which type of pill would you prefer for this healthy newly married girl without any contraindications for OCPs? • Estrogen dose • Type of progesterone • Mono/triphasic
Estrogen in OCPs • Low dose • V.low dose
Progestins in Oral Contraceptives 19-Nortestosterone Spironolactone • Drospirenone Estranes Gonanes • Norethindrone • Norethindrone acetate • Ethynodioldiacetate • Norethynodrel • Lynestrenol • Levonorgestrel • Norgestrel • Desogestrel • Norgestimate • Gestodene *Not available in the United States. Adapted from Sulak PJ. OBG Management. 2004;Suppl:3-8.
Phasic Combination Oral Contraceptives • Triphasic oral contraceptives contain increasing doses of estrogen or progestin throughout the menstrual cycle in order to decrease adverse events • A Cochrane review of triphasic and monophasic oral contraceptives found: • Comparable efficacy • Suggestion of less spotting, breakthrough bleeding, and amenorrhea with triphasic oral contraceptives van Vliet HA, et al. Cochrane Database Syst Rev. 2006;3:CD003553.
Case • A 42 yr old woman on 20 micgm EE pill for last 2 months comes to you with breakthrough bleeding. • Expressing concern about ocpills in general & at her age in particular • Overall health good,non smoker,no CVS risk factors,normotensive, BMI 25
How would you approach her breakthrough bleeding? • Breakthrough bleeding….. DEFINITION? • E ? P ? • 21/7 vs 24/4 vs extended cycle
bleeding that is unscheduled, that occurs outside the time of the hormone-free interval, and also is not within the first 3 to 4 days of active pills within a given OC cycle. Currently, many people feel that the better term to use is 'unscheduled bleeding.'between 10% and 30% of women will have some spotting in the first 2 months of OC use. The high proportion of the spotting or abnormal bleeding will usually disappear by the third month.
Women Who Have an Increased Risk of Breakthrough Bleeding • Any woman beginning a new form of hormonal contraception • Women who inconsistently use oral contraceptives or miss doses • Oral contraceptive users who have chlamydial cervicitis and/or endometritis • Infection is the likely cause when breakthrough bleeding appears several months after initiating an oral contraceptive regimen • Smokers, possibly because of fluctuations in estrogen levels • Vomiting or diarrhea • Taking anticonvulsants or rifampicin Wallach M, et al., eds. Modern Oral Contraception: Updates from The Contraception Report. 2000.
Weight Gain Nausea Mood Changes Headaches Breast Tenderness Irregular Bleeding Side Effects Cited for Discontinuation of Oral Contraceptives % Discontinuing Rosenberg MJ, et al. Am J Obstet Gynecol. 1998;179:577-582.
Case • A 20-year-old woman would like to begin OC use, but has an older sister whose severe migraine headaches began when she started OC use. The patient reports a personal history of mild headaches occurring 6 to 8 times yearly for the past 4 years. These last 3 to 4 hours and are bilateral, pressing, or tightening in quality, and not associated with nausea, vomiting, photophobia, or phonophobia. The headaches respond well to over-the-counter medications such as NSAIDs. Her neurologic examination is normal and there are no other contraindications to OC use.
Evidence and Guidelines • Safety. There is no evidence that TTH is a risk factor for the development of ischemic stroke. • Tolerability. There is no evidence that hormonal fluctuations play a role in the pathogenesis or clinical course of TTH. There is modest evidence that a family history of migraine increases the risk of developing headache on OCs. • Guidelines. TTH is not considered a contraindication to OC use by any professional guidelines.
Recommendations • While the presence of TTH does not contraindicate OC use in this patient, the strong family history of migraine does increase the risk that she will develop new-onset migraine with OC use • weighing the potential benefits of OC use and the strength of other reasons for OC use against the small but real risk of headache precipitation
Case • A 23-year-old woman has severe dysmenorrhea that has been unresponsive to treatment with NSAIDs. She has migraine without aura and takes sodium valproate 250 mg twice daily for migraine prevention. Because she desires contraception, OCs have been recommended as treatment of dysmenorrhea. The patient has heard through friends and the popular press that because she has migraine she should not use OCs. Her neurologic examination is normal and she has no other contraindications to OC use.
Safety.Migraine and OC use are both risk factors for ischemic stroke. The risk of stroke in childbearing age women is low, but good quality evidence suggests that a diagnosis of migraine without aura increases this risk by a factor of about 3. The combination of migraine and OC use increases the risk of stroke by a factor of about 14. Stroke risk appears to be higher with OCs containing high doses of estrogen (greater than 50 µg of ethinyl estradiol).
Interestingly, migraine appears to be a risk factor for stroke only in women under the age of 45.
Tolerability. OCs are widely believed to cause or aggravate headache, but the evidence that this is a common or clinically significant problem is remarkably slim. • Regardless of cause, headache occurring in association with OC use tended to improve despite continued OC use.
Migraine in women using traditional COCs is more likely to occur during the pill-free week, presumably triggered by estrogen withdrawal. • OCs containing lower levels of estrogen may be less likely to provoke headache • There is no evidence that the dose or type of progestin in an OC has an important influence on headache
Guidelines. • World Health Organization (WHO) and American College of Obstetrics and Gynecology (ACOG) guidelines consider that for women under the age of 35 who have migraine without aura, and few or no cardiovascular risk factors, the benefits of OC use typically outweigh the risks
The International Headache Society task force on combined OCs and hormone replacement therapy in women with migraine concluded that "there is no contraindication to the use of COCs in women with migraine in the absence of migraine aura or other risk factors.
Recommendations • This patient has migraine without aura, is under 35, has no additional risk factors for stroke, and is likely to experience important improvement in another condition from OC use. Avoidance of unintended pregnancy is especially important in this patient because she is taking valproate, a known teratogen.For her, the benefits of OC use probably outweigh the drawbacks, and this assessment is supported by professional guidelines.
It would be wise to obtain a baseline assessment of the frequency, severity, and character of this patient's headaches and then monitor their frequency and severity while she is using OCs.
Contraception During Perimenopause: Oral Contraceptives *Percentage of women experiencing unintended pregnancy with typical use within first year of use. Grimes DA, Wallach M, eds. Modern Contraception: Updates from The Contraception Report. 1997; Hatcher RA, Nelson AL. In: Contraceptive Technology. 2004:391-460.
Effect of a Low-Dose Oral Contraceptive (Minestrin™) on Menses During Perimenopause* • Shortened menstrual cycle • Decreased variability in menses • Less severe bleeding • Reduced incidence and duration of clotting/flooding *Minestrin™ = 20 µg of ethinyl estradiol plus 1 mg of norethindrone acetate Casper RF, et al.Menopause. 1997;4:139-147.
*P<0.01 NS=not significant Placebo 20-g EE/1-mg NETA * * * Change from Baseline (%) NS Sexual Psychosocial Global Physical Effect of a Low-Dose Oral Contraceptive (Minestrin™) on Quality of Life During Perimenopause Endpoint in Menopause-Specific Quality-of-Life Questionnaire EE = ethinyl estradiol; NETA = norethindrone acetate Reproduced with permission from Casper RF, et al. Menopause. 1997;4:139-147.
105 100 95 90 85 80 75 0 6 12 18 24 30 36 Oral Contraceptives Maintain Bone Mass in Women Aged 41–49 Years % Bone Mass Reference Standard Oral Contraceptives Control Months of Use Shargil AA. Int J Fertil. 1985;30:15-28.
Stopping Oral Contraceptives or Transitioning to Hormone Therapy for Menopause • Determine when an oral contraceptive is no longer needed • Measure follicle-stimulating hormone and/or estradiol levels after being off of oral contraceptives for 2 weeks • Serial elevations in follicle-stimulating hormone levels indicate menopause in most women • Estimate age of menopause based on onset of perimenopausal symptoms • Arbitrarily stop between the ages of 50 and 52 • Transition to hormone therapy may be indicated in some women
Types of Premenstrual Disorders • Premenstrual molimina • Normal premenstrual discomfort, nonproblematic • Most common premenstrual disorder • Premenstrual Syndrome (PMS) • Bothersome adverse somatic and/or affective symptoms during the luteal phase • Premenstrual Dysphoric Disorder (PMDD) • Significant impairment • Least common premenstrual disorder Ginsburg KA, Dinsay R. In: Ransom SB, ed. Practical Strategies in Obstetrics and Gynecology. Philadelphia: W.B. Saunders Company; 2000:684-694; Kessel B. Obstet Gynecol Clin North Am. 2000;27:625-639.
ACOG Diagnostic Criteria forPremenstrual Syndrome* • Other disorders must be excluded • Must include dysfunction in social or economic performance • Symptoms must be present in the absence of pharmacologic therapy, hormone ingestion, or drug or alcohol use ACOG=American College of Obstetricians and Gynecologists *Limited core of symptoms; †Hallmark affective symptom Adapted from ACOG Practice Bulletin No. 15. Obstet Gynecol. 2000;95(4): supplemental material at end of issue.
Premenstrual Dysphoric Disorder:Symptoms and DSM-IV Criteria • Must have ≥ 5 symptoms, including at least 1 core symptom • Symptoms must occur during the last week of the luteal phase • Symptoms are relieved within a few days of starting menses American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association, 2000.
Validated Tests for Diagnosing PMS and PMDD PMS=premenstrual syndrome; PMDD=premenstrual dysphoric disorder Feuerstein M, Shaw WS. J Reprod Med. 2002;76:279-289; Steiner M, et al. Arch Women Ment Health. 2003;6:203-209; Steiner M, et al. J Affect Disord. 1999;53:269-273; Endicott J, et al. Arch Womens Ment Health. 2006;9:41-49.
Therapies for Premenstrual Syndrome • Lifestyle changes • Aerobic exercise • Dietary modification • Cognitive-behavioral therapy • Pharmacologic agents • Selective serotonin reuptake inhibitors (SSRIs) • The SSRIs that have an FDA-approved indication for treating premenstrual dysphoric disorder are: • Fluoxetine hydrochloride • Sertraline hydrochloride • Paroxetine hydrochloride • Spironolactone • Anxiolytics • Gonadotropin-releasing hormone (GnRH) agonists • Hormonal contraceptives ACOG Practice Bulletin No. 15. Obstet Gynecol. 2000;95(4): supplemental material at end of issue.