Download
1 / 54
540 likes | 565 Views
Explore the polarized views on surgical versus physical therapy treatments for subacromial pain. Examine the rise in surgeries and the poor evidence supporting interventions. Understand the pathology, acromial morphology, rotator cuff mechanics, and tendon homeostasis.

E N D
Controversies in the Management of Subacromial Impingement Yemi Pearse MA (Oxon) FRCS(Orth) Consultant Orthopaedic Surgeon The London Shoulder Partnership Shoulder Unit St George’s Hospital 16th November 2016 www.thelondonshoulderpartnership.co.uk
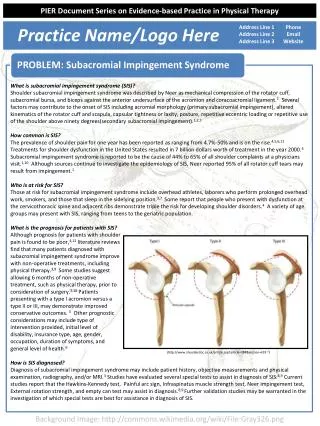
Subacromial impingement / Subacromial pain syndrome Most common presentation of pain and dysfunction in middle age shoulder but treatment is controversial Conflict between advocates of surgery and advocates of physical therapy for management of subacromial pain Polarized views regarding efficacy of either
Ketola S, Lehtinen J, Arnala I, Nissinen M, Westenius H, Sintonen H, Aronen P, Konttinen YT, Malmivaara A, Rousi T. Does arthroscopic acromioplasty provide any additional value in the treatment of shoulder impingement syndrome?: a two-year randomised controlled trial. JBJS(Br) October 2009 Arthroscopic acromioplasty provides no clinically important effects over a structured and supervised exercise programme alone in terms of subjective outcome or cost-effectiveness when measured at 24 months. Structured exercise treatment should be the basis for treatment of shoulder impingement syndrome, with operative treatment offered judiciously until its true merit is proven.
Controversy 2.5-fold increase in 10 years between 1996 and 2006 in number of acromioplasties performed in New York In last 10 years in UK 746% increase in arthroscopic subacromial decompression Excellent results in cohort studies for both surgery and physical therapy
The problem Poor understanding of pathology Poor real evidence for all interventions - no placebo controlled trials (ethics and practicality)
A painful condition resulting from impingement of the rotator cuff under the coracoacromial arch. Neer 1972. Ache at anterolateral border of acromion radiating to upper arm Pain is worse with overhead activity or repetitive work Painful arc on elevation of the arm
Neer described 3 stages of impingement syndrome • Oedema and haemorrhage of the bursa and cuff (patients less than 25 years old) - No surgery required • Irreversible changes such as fibrosis and tendinitis of the rotator cuff (25 to 40 years old) – bursectomy and CAL division after 18 months of conservative treatment (acromioplasty usually not required) • More chronic changes (eg partial or complete tears) associated with type III acromion - anterior acromioplasty
Difference in acromial morphology noted as early as 1875 by Hamilton and 1909 by Goldthwaite Bigliani 1986 139 cadaver shoulders 3 types of acromial morphology • Flat (17%) • Curved (43%) • Hooked (40%)
- No correlation between acromial shape and cuff pathology - Progression to cuff tear cannot be from acromial abrasion as most partial thickness tears are joint side or intrasubstance - No evidence of inflammatory cells and “tendinitis” on histological evaluation
Rotator cuff muscles (in particularly supraspinatus) create a virtual centre of rotation for glenohumeral motion Upward vector force (deltoid) is converted to a turning moment as deltoid acts around virtual centre of rotation
Cuff deficiency will result in proximal humeral migration due to reduced opposition to pull of deltoid
In vivo (load bearing static xrays) humeral head remains centred on elevation in normal subjects but rises in patients with rotator cuff pathology In vivo (video fluoroscopy) humeral head rises between 45o and 90o in healthy subjects with fatigue Dynamic ultrasound shows that the CAL bulges in rotator cuff disease Wang et al. Ultrasound Med Biol 2009
CAL is poorly named • not a ligament but a retinaculum • increases efficiency of muscle pull by avoiding bowstringing • Contact between supraspinatus and coracoacromial arch is inevitable and probably desirable • BUT compression of the tendon is bad
Tendon homeostasis Repair Damage
Tendon homeostasis TIMPs MMPs
Tendinosis Damage Repair
Tendinosis Appropriate mechanical loading results in homeostasis Inappropriate loading results in upregulation of MMPs and catabolic cytokines no mechanical stimulus (tendons need tensile load) excessive mechanical stimulus (too much tensile load) compression (tendons hate compressive load) Thornton et al. Br J Sports Med 2008
Tendinosis Absence of inflammatory cells Tenocytes change characteristics - Change in N:C ratio - Change in EM composition - Become secretory rather than synthesizing cells Note fibre disorientation Efficiency of load transmission from muscle to bone declines
Supraspinatus has greater susceptibility than rest of rotator cuff - Compressive forces from coracoacromial arch - Isometric (unlike internal and external rotators) therefore greater interface stresses
Supraspinatus works harder Poor load transmission Failure of tendon homeostasis - TENDINOPATHY
Supraspinatus works harder Poor load transmission Pathological tensile load on tendon Failure of tendon homeostasis - TENDINOPATHY
Supraspinatus works harder Poor load transmission Failure of tendon homeostasis - TENDINOPATHY Tendon compressed against CAL Muscle fatigues more quickly Humeral head rises with abduction/ elevation Narrowing of acromiohumeral distance
Supraspinatus works harder Poor load transmission Pathological tensile load on tendon Failure of tendon homeostasis - TENDINOPATHY Tendon compressed against CAL Muscle fatigues more quickly Humeral head rises with abduction/ elevation Narrowing of acromiohumeral distance
Support by other cuff Increase aerobic capacity Supraspinatus works harder Poor load transmission Pathological tensile load on tendon Failure of tendon homeostasis - TENDINOPATHY Tendon compressed against CAL Increased elasticity in CAL Muscle fatigues more quickly Humeral head rises with abduction/ elevation Narrowing of acromiohumeral distance
Support by other cuff - Pain inhibition - Supraspinatus works harder Poor load transmission Pathological tensile load on tendon Failure of tendon homeostasis - TENDINOPATHY Tendon compressed against CAL PAIN Muscle fatigues more quickly Humeral head rises with abduction/ elevation Narrowing of acromiohumeral distance
Support by other cuff E - Pain inhibition - Supraspinatus works harder A Poor load transmission Pathological tensile load on tendon Failure of tendon homeostasis - TENDINOPATHY D Tendon compressed against CAL PAIN Muscle fatigues more quickly Humeral head rises with abduction/ elevation B Narrowing of acromiohumeral distance C -
A – Supraspinatus works harder Reduce work of suprapsinatus by addressing - Capsular restriction - Glenohumeral instability - Poor scapular control - Poor kinetic chain / core strength - Poor trunk rotation
Increase “travel distance” by: • Rotation of trunk • Medialisation of scapula • External rotation of shoulder
With decreased travel distance shoulder muscles have to work harder to achieve same angular velocity
Support by other cuff Increase aerobic capacity B – Muscle fatigues Supraspinatus works harder Poor load transmission Failure of tendon homeostasis - TENDINOPATHY Often adaptive changes have already occurred and aerobic conditioning exercises can be “flogging a dead horse” Offload supraspinatus by addressing • Inappropriate technique • Inappropriate activities • (Inadequate conditioning) Tendon compressed against CAL Muscle fatigues more quickly Humeral head rises with abduction/ elevation Narrowing of acromiohumeral distance
C – Narrowing of acromiohumeral distance Address posteroinferior capsular restriction • Posterior capsule stretches • Sleeper stretches
C – Narrowing of acromiohumeral distance Address scapular dyskinesia Scapula rotates during abduction 2.5 to 24 degrees GH:ST ratio = 4.3:1 24 degrees to full abduction GH:ST ratio = 5:4 Abnormal GH:ST ratio narrows outlet
D – Tendinopathy Orthobiologics • PRP • Autologous blood • Growth factors “Mechanomodulators” • ECSWT • Needling
E – Pain inhibition Acupuncture Analgesia and NSAIDs Steroid injection
Accurate assessment and tailored therapy One size does not fit all and multiple potential ways to “break the vicious cycle” Need to have been alive long enough to develop tendon degeneration and impingement is almost always secondary in young and in absence of structural lesion correctable
Support by other cuff E - Pain inhibition - Supraspinatus works harder A Poor load transmission Pathological tensile load on tendon Failure of tendon homeostasis - TENDINOPATHY D Tendon compressed against CAL PAIN Muscle fatigues more quickly Humeral head rises with abduction/ elevation B Narrowing of acromiohumeral distance C -
Support by other cuff E - Pain inhibition - Supraspinatus works harder A Poor load transmission Break vicious circle Escape from tendinopathy to tendon homeostasis Pathological tensile load on tendon Failure of tendon homeostasis - TENDINOPATHY D Tendon compressed against CAL PAIN Muscle fatigues more quickly Humeral head rises with abduction/ elevation B Narrowing of acromiohumeral distance C -
Accurate assessment and tailored therapy 4 mechanical techniques applied sequentially while patient performs the activity or movement that most closely reproduces their symptoms 1. Techniques to reduce the thoracic kyphosis 2. Scapular positioning techniques 3. Humeral head positioning procedures 4. Pain and symptom neuromodulation procedures
Accurate assessment and tailored therapy 4 mechanical techniques applied sequentially while patient performs the activity or movement that most closely reproduces their symptoms Identifying technique(s) that reduce symptoms Focus on these
Judicious use of steroid injection Action unknown Long acting pain killer – stop pain inhibition Anabolic effect on supraspinatus and other cuff muscles (kick start versus temporary boost) I only ever give one
Surgery is for when therapy fails Accept humeral head will migrate proximally Accommodate this with subacromial decompression • Reduces compression on tendon • Breaks vicious cycle Continue to optimise adaptive changes
With this approach controversy is artificial Comparative studies are meaningless and miss the point No placebo controlled trials for either operative or non-operative treatment but numerous cohort studies Recommend • Detailed assessment • Shoulder symptom modification procedure • Surgery if correctables corrected but symptoms persist
Clinical assessment Age (usually 40 +) Anterosuperior pain “in the muscle” Weakness may be present but is secondary to pain and should resolve if pain is abolished Apparent stiffness may also be secondary to pain Clinical tests lack sensitivity and specificity
Clinical assessment Neer 75% to 97% sensitivity 30% to 50% specificity reported Hawkins 92% sensitivity 25% to 45% specificity reported Kessel and Watson painful arc 30% to 97% sensitivity 10% to 80% specificity reported