Download
1 / 29
320 likes | 627 Views
Epilepsy Surgery. E Feoli MD North East Regional Epilepsy Group 2012. Comprehensive Epilepsy Center. Referrals. Evaluation: ●History/Exam ●EEG ●Imaging. Controlled. Not Controlled. Video-EEG. Epilepsy. Non-epileptic Events. Refer. Medical Management. Surgical Management.

E N D
Epilepsy Surgery E Feoli MD North East Regional Epilepsy Group 2012
Comprehensive Epilepsy Center Referrals Evaluation: ●History/Exam ●EEG ●Imaging Controlled Not Controlled Video-EEG Epilepsy Non-epileptic Events Refer Medical Management Surgical Management
The Poorly Controlled, Intractable Seizure Patient Despite medical management, patient continues to have frequent, debilitating seizures Commonly on polytherapy (more than one medication)
Candidates for Epilepsy Surgery • Persistent seizures after initial attempts at treatment (at least 2 appropriate AEDs at reasonable doses) • Impaired quality of life due to ongoing seizures • For focal resection: single seizure focus that can be safely removed • Palliative procedures: corpus callosotomy, subpial transections, VNS, others
Epilepsy Surgery To determine where the seizures are coming from Video-EEG monitoring MRI MRS: PET: SPECT:
Goals of Video-EEG Monitoring Epilepsy vs. non-epileptic events Characterize epilepsy type Pre-surgical evaluation FOCAL EPILEPSY
EEG Slide 99-10-31/ROUTINE
Epilepsy Surgery To make sure that it is safe Wada test: to study speech and memory Neuropsychological testing: mental functions (IQ, memory, attention) and personality assessment Psychological evaluation Ophthalmologic evaluation
Epilepsy Surgery Some cases in which the localization is not clear or where function could be affected will require INVASIVE ELECTRODES Depth electrodes Subdural electrodes
Types of Epilepsy Surgery Temporal Lobectomy Extratemporal Resections Hemispherectomy Corpus Callosotomy
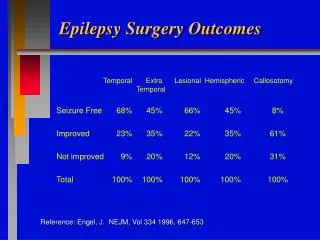
Outcome after epilepsy surgery Anterior temporal lobectomy 70-80% seizure free Neocortical resection With lesion: 50-80% seizure free Without lesion: 30-50% seizure free Hemispherectomy Significant improvement Corpus Callosotomy Significant improvement for drop attacks
Complications of surgery Low rate of complications Infections Bleeding Anesthesia Function
Vagus Nerve Stimulator (1997) Intractable epilepsy patient without focus or desires interim step before epilepsy surgery Goal is to reduce amount/severity of seizures vs. cure Device surgically implanted in left chest/axilla area Coils around left vagus nerve Stimulation is automatic; patient can additionally stimulate device if aura
VNS Therapy • VNS: <10% seizure free, • 30-50% with at least 50% seizure decrease, more with lesser improvement; effects on seizure severity?
Conclusion -Not all patients with refractory epilepsy are surgical candidates. -Patients with FOCAL refractory epilepsy are candidates for surgery. -Multiple steps are required before your doctor concludes that you are a surgical candidate. -
Conclusion You might be a good surgical candidate however a RESECTIVE procedure might not be possible, due to the proximity o the seizure focus to “eloquent cortex”