Download
1 / 58
810 likes | 1.92k Views
Bone Health and Osteoporosis Center Metabolic Bone Diseases and Mineral Disorders. SECONDARY CAUSES OF OSTEOPOROSIS. Nelson B. Watts, MD. SECONDARY CAUSES OF OSTEOPOROSIS. Use of bone densitometry Secondary causes of bone loss Laboratory evaluation Calcium and vitamin D

E N D
Bone Health and Osteoporosis Center Metabolic Bone Diseases and Mineral Disorders SECONDARY CAUSES OF OSTEOPOROSIS Nelson B. Watts, MD
SECONDARY CAUSES OF OSTEOPOROSIS • Use of bone densitometry • Secondary causes of bone loss • Laboratory evaluation • Calcium and vitamin D • Bone turnover markers • Lateral spine imaging with DXA
DEFINITION OF OSTEOPOROSIS • A skeletal disorder characterized by • compromised bone strength predisposing to • an increased risk of fracture. • Bone strength reflects the integration of two main features: • bone density and • bone quality. Normal Bone 2000 NIH Consensus Development Conference Osteoporotic Bone
Category T-score Normal -1.0 and above Low bone mass (osteopenia) Between -1.0 to -2.5 Osteoporosis -2.5 and below Kanis JA et al, J Bone Miner Res 1994;9:1137-1141 WHO CRITERIA FORPOSTMENOPAUSAL OSTEOPOROSIS The T-score compares an individual’s BMD with the mean value for young normal individuals and expresses the difference as a standard deviation score.
WHY THE WHO CHOSE T = -2.5 • "When measurements are made at the hip alone, …the prevalence [of osteoporosis] is about one in five white women, comparable to the lifetime risk of a single osteoporotic fracture, such as a hip fracture.“ • "Such a cutoff value identifies approximately 30% of postmenopausal women as having osteoporosis using measurements made at the spine, hip, or forearm. This is approximately equivalent to the lifetime risk of fracture at these sites." Kanis JA, et al. J Bone Miner Res 1994; 9:1137-1141
BONE DENSITY MEASUREMENTS AT PERIPHERAL SITES LIMITATIONS • Less predictive for hip fracture than hip measurement • Cannot be used for diagnosis with WHO criteria • Cannot be used for monitoring (sites less likely to change) QUS DXA pQCT ADVANTAGES • Portable • Less expensive than central DXA • Ultrasound does not involve radiation
PREVALENCE OF OSTEOPOROSIS ANDLIFETIME FRACTURE RISK IN WHITE WOMEN 1 2 Percent 1. Melton LJ III, et al. J Bone Miner Res 1995;10:175 2. Melton LJ III, et al. J Bone Miner Res 1992;7:1005
Missed 55% 66% 84% 90% PREVALENCE OF OSTEOPOROSIS VARIES BY SITE AND METHOD NORA Study, 200,160 ambulatory women age 50 and older Percent of subjects 2.5 SD or more below young adult mean *Estimated from NAHNES III Siris E et al, JAMA 2001;286:2815-2822
AGE DEPENDENCE OF T-SCORES Data from manufacturers' data bases T-score Age (years) Faulkner KG et al. J Clin Densitom 1999;2:343
WHO CRITERIA • Apply only to postmenopausal Caucasian women • not men, younger women, other ethnic groups • Apply only PA spine, hip and forearm DXA • not lateral spine, heel, finger, etc • Apply only for central DXA • not peripheral DXA, QCT, QUS, etc.
FEMALE OLDER AGE EARLY MENOPAUSE FAMILY HISTORY FAIR SKIN NULLIPARITY SLENDER BUILD LOW CALCIUM INTAKE SMOKING INACTIVITY RISK FACTORS FOR OSTEOPOROSIS
36% did have osteoporosis 64% did not have osteoporosis 48% had no risk factors 67% had no risk factors 52% had one or more risk factors 33% had one or more risk factors RISK FACTORS AND LOW BMD IMPACT Trial • ~7,000 women in 21 countries without known osteoporosis had BMD testing and riskfactor assessment ~50% of patients with osteoporosis ..did not have risk factors ~50% of patients with risk factors did ..not have osteoporosis Watts NB et al, Arthritis Rheum 2001;44:S256
WHO SHOULD HAVE ABONE DENSITY TEST? U.S. Preventive Services Task Force • Women 65 years of age and older [should] be screened routinely for osteoporosis • Routine screening [should] begin at 60 years of age for women at increased risk for osteoporotic fractures • Low body weight (<70 kg) • Lack of estrogen • Possibly other risk factors • No recommendation for or against screening younger women at high risk US PSTF, Ann Intern Med 2002;137:526-528
WHO SHOULD HAVE ABONE DENSITY TEST? Number Needed to Screen Number Needed to Treat Fracture Type Fracture Type Age Age Nelson HD et al, Ann Intern Med 2002;137;529-541
WHO SHOULD HAVE ABONE DENSITY TEST? ISCD OsteoFLASH, www.iscd.org
FDA-APPROVED MEDICATIONSEVIDENCE FOR FRACTURE REDUCTION Evidence for effect but not an FDA-approved indication
NOF TREATMENT GUIDELINES 2008 www.nof.org
NOF GUIDE -- 2008 Postmenopausal women and men age 50 and older presenting with the following should be treated: • A hip or vertebral (clinical or morphometric) fracture • BMD T-score ≤ -2.5 at the femoral neck, total hip or spine after appropriate evaluation to exclude secondary causes • Low bone mass (T-score between -1.0 and -2.5 at the femoral neck, total hip or spine) AND • 10-year probability of hip fracture ≥3% or • 10-year probability of any major osteoporosis-related fracture* ≥20% based on the US-adapted WHO algorithm *Hip, humerus, forearm or clinical vertebral fracture
T-score -2.5 or below in the femoral neck, total hip or spine A fracture of the hip or vertebra (clinical or morphometric) T-scores between -1.0 and -2.5 10-year risk ≥3% for hip fracture or ≥20% for major osteoporotic fractures based on FRAX™ model NOF GUIDELINES 2008 After exclusion of secondary cause, treat postmenopausal women and men age 50 and older who have…
Mary Smith, 66.8 years old Wt. 140 lbs., Ht 64 in. FN T-score -2.4, no risk factors www.shef.ac.uk/FRAX
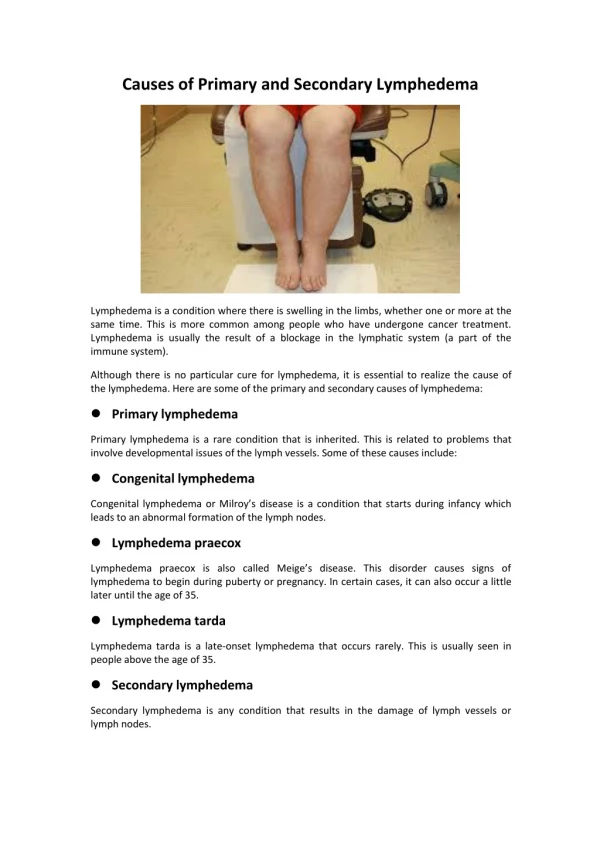
EVALUATION OF PATIENTS WITH OSTEOPOROSIS • Just because a woman is postmenopausal and has osteoporosis doesn’t mean that she has postmenopausal osteoporosis • Failure to identify underlying disorders may result in inadequate or inappropriate treatment
SOME CAUSES OF SECONDARY OSTEOPOROSIS IN ADULTS Adapted from Hodgson SF and Watts NB, AACE Guidelines on Osteoporosis, www.aace.com
ENDOCRINE AND METABOLIC DISEASES ASSOCIATED WITH OSTEOPOROSIS • Hypogonadism • Hypercalciuria • Hyperthyroidism • Hyperparathyroidism • Cushing’s syndrome • Acromegaly • Growth hormone deficiency
NUTRITIONAL CONDITIONSASSOCIATED WITH OSTEOPOROSIS • Vitamin D deficiency • Calcium deficiency • Vitamin B12 deficiency • Weight loss • Malabsorption • Gastric surgery • Anorexia nervosa • Chronic liver disease • Alcoholism • Malnutrition • Prolonged TPN
DRUGS ASSOCIATED WITH OSTEOPOROSIS • Glucocorticoids • Anti-epilepsy drugs • Thyroid hormone (supraphysiologic doses) • Depo-Provera • GnRH agonists • Aromatase inhibitors • TZDs • SSRIs • PPIs
DISORDERS OF COLLAGEN METABOLISM • Osteogenesis imperfecta • Homocystinuria • Ehlers-Danlos syndrome • Marfan syndrome
OSTEOGENESIS IMPERFECTA Type I • Autosomal dominant inheritance • Decreased production of type I procollagen; substitution for glycine in triple helix of 1(I) • Normal stature • Little or no deformity • Blue sclerae • Hearing loss in 50% • Teeth are usually normal • Histomorphometry: increased cortical osteocytes, woven bone, thin collagen bundles
OSTEOGENESIS IMPERFECTA Type IV • Autosomal dominant inheritance • Point mutation in 2(I) chain • Normal sclerae • Mild to moderate deformity • Variable short stature • Hearing loss in some • Dentogenesis imperfecta is common
OTHER CAUSES OF LOW BONE MASS • Rheumatoid arthritis • Inflammatory bowel disease • COPD • Organ transplantation • Immobilization • Multiple myeloma • Some cancers • Renal tubular acidosis • Gaucher’s disease • Mastocytosis • Thalassemia
Post-menopausal women over age 65 BMD T-score -2.5 or below (n=664) No previous known contributors to History of known medications or diseases osteoporosis based on past medical history affecting bone and mineral metabolism (n=309) (n=355) Ineligible subjects Incomplete laboratory testing (n=136) SECONDARY CAUSES OF OSTEOPOROSIS Eligible subjects Complete battery of laboratory tests available (n=173) Tannenbaum C et al, J Clin Endocrinol Metab 2002;87:4431-4437
SECONDARY CAUSES OF OSTEOPOROSIS Patients with at least 1 new diagnosis (n=84) 48.6% Vitamin D deficiency, <20 ng/mL (n=35) 20.2% Hypercalciuria 9.8% Renal (n=7) Idiopathic (n=6) Undefined (n=4) Malabsorption 8.1% Relative calcium malabsorption (n=11) Celiac sprue (n=3) Hyperparathyroidism 6.9% Primary (n=1) Secondary (n=11) Exogenous hyperthyroidism (n=4) 2.3% Cushing’s disease (n=1) 0.6% Hypocalciuric hypercalcemia (n=1) 0.6% Tannenbaum C et al, J Clin Endocrinol Metab 2002;87:4431-4437
LABORATORY EVALUATION FOR OSTEOPOROSIS Abnormal 24-h urine calcium for all 39/173 Serum 25-OH vitamin D for all 35/173 Serum calcium for all 3/173 Serum TSH for all on replacement 4/25 This strategy finds 98% of cases, costs $116 per patient screened, $332 per case found Tannenbaum C et al, J Clin Endocrinol Metab 2002;87:4431-4437
VITAMIN D STATUS • Best reflected by serum 25-hydroxyvitamin D levels • Lab reference range is 20-100 ng/mL • Minimum desirable level is 30 ng/mL (80 nmol/L) • Reasonable range is 30 to 60 ng/mL (80 to 150 nmol/L)
VITAMIN D REDUCES RISK OF FALLING Meta-Analysis Bischoff-Ferrari HA et al. JAMA 2004;291:1999-2006
VITAMIN D REDUCES FRACTURESAND MAY REDUCE MORTALITY Vitamin D 100,000 IU Q 4 months or placebo N=2037 men and 649 women ages 65-85 Fractures (hip, wrist, forearm, vertebra) Survival OR 0.78 (0.61,0.99) OR 0.88 (0.74,1.06)) Trivedi DP et al, BMJ 2003;326-469-475
MOST OF US WILL BENEFIT FROM A VITAMIN D SUPPLEMENT • Vitamin D has important skeletal and extra-skeletal effects • Adequate 25-hydroxyvitamin D level is ≥30 ng/dL • Vitamin D deficiency is common • Most patients require 1,000-2,000 IU vitamin D per day to achieve an adequate level • “Safe upper limit” is 2,000 IU per day • Supplements of 1,000 IU tablets are now widely available (1,000-2,000 IU daily • Rx 50,000 IU ergocalciferol may be required (weekly, every other week)
OPTIMAL CALCIUM INTAKE 1200 mg daily for adults age 50 and older TOTAL FROM ALL SOURCES Average calcium from diet: Women 50 and older : ~500 mg daily Men 50 and older: ~600 mg daily Most people need a calcium supplement of 700 to 1000 mg daily. Many people are taking too much.
24-HOUR URINE CALCIUM • Lab reference range 100-300 mg/day • Typical is 2-3 mg/kg/day • Upper limit of “normal” is 4 mg/kg/day • Wt 100 kg, normal up to 400 mg/day • Wt 50 kg, normal up to 200 mg/day • Low urine calcium = low intake or malabsorption • High urine calcium = high intake or calcium wasting Must be collected when vitamin D is adequate and calcium intake is within target of 1200-1500 mg daily
LABORATORY EVALUATION FOR OSTEOPOROSIS • CBC • Chemistry panel and phosphorus • 25-hydroxyvitamin D • 24-hour urine for calcium and creatinine • If patient is male, serum testosterone (total and free) • Other studies if indicated by history, physical findings or initial laboratory results
BIOCHEMICAL MARKERS OF BONE TURNOVER • Enzymes (alkaline phosphatase, acid phosphatase) • Degradation products (hydroxyproline, collagen cross links) • Byproducts(osteocalcin, procollagen I extension peptides)
N-TELOPEPTIDE REGION C-TELOPEPTIDE REGION HELICAL REGION CTx NTx Pyr Dpd COLLAGEN CROSS LINKS Watts NB. Clin Chem 1999;45:1359-1368
CTX 4.8 4.1 Free DPD 2.2 1.9 High Marker Both BMD AND MARKERS PREDICT HIP FRACTURETHE EPIDOS STUDY 6 5 4 Odds Ratio 2.7 3 2 1 0 Low Hip BMD Garnero P et al, J Bone Miner Res 1996;11:1531
NOT EVERYONE WITH OSTEOPOROSIS HAS ABNORMAL BONE TURNOVER 89 Elderly Women with Osteoporosis Pyr Dpd NTx Garnero P et al, J Clin Endocrinol Metab 1994;79:1693
URINE NTX • Remodeling has diurnal variation: need second morning fasting urine or fasting blood • Urine sample may be preferred for logistical reasons Target: at or below the median value for premenopausal women (30 nmol BCE/mmol creatinine)* *de Papp AE et al, Bone 2007;40:1222-1230
CLINICAL USES FOR BONE TURNOVER MARKERS • Patient with borderline low BMD who is not a treatment candidate: when to test again • Patient with low BMD who has no other risk factors: when to treat • Patient on antiresorptive treatment who has bone loss or fracture: is the medication being absorbed and is it working? • Patient on anabolic therapy: is medication working?