Download
1 / 46
460 likes | 616 Views
The Eye Lids. Prof. Dr. Rengin Yıldırım. Normal Anatomy. Both the upper & lower eyelids have similar structure They consist of an anterior lamella (skin & orbicularis muscle) and a posterior lamella (tarsal plate & conjunctiva).

E N D
The Eye Lids Prof. Dr. Rengin Yıldırım
Normal Anatomy • Both the upper & lower eyelids have similar structure • They consist of an anterior lamella (skin & orbicularis muscle) and a posterior lamella (tarsal plate & conjunctiva)
The orbital septum extends from the orbital rim and separates the preseptal orbicularis muscle from the preaponeurotic fat pad. • The lid retractors lie between the preaponeurotic fat pad and the globe.
Lid Retractors • The upper lid retractors consist of levator palpebra superior muscle and its aponeurosis and the superior tarsal muscle (Muller’s muscle) • The lower lid retractors arise from the sheat of the inferior rectus muscle and are similarly composed of aponeurosis and the inferior tarsal muscle
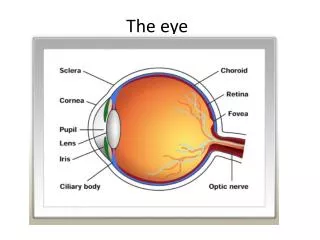
The gray line divide s eye lid margin into anterior and posterior parts Eye lashes, moll & zeis glands orifices takes place at the front part Meibomian gland orifices are placed behind the gray line. The structure eye lid margin
Disorders of the eye lashes • Trichiasis:Posterior misdirection of eye lashes from their normal sites of origin. • Metaplastic lashes: which originate from the meibomian gland orifices
Distichiasis in which partial or complete second row of lashes arises from or behind the meibomian gland orifices
Madorosis is decrease in number or complete loss of lashes • Poliosis Premature whitening of lashes sometimes may involve eye brows
Blepharitis • Common bilateral symmetrical condition • Anterior form is usually because of stayphlococcal infection in sebborrhoeic patients • Posterior form is associated with meibomian gland dysfunction (ocular rosasea)
Entropion • Entropion or inversion of the lid margin may be congenital and acquired. • The acquired variety can be the result of ageing changes (involutional entropion) or the cicatricial changes (cicatricial entropion)
Pathogenesis of Senile Entropion • Horizontal Lid Laxity as well as medial and lateral tendon laxity • Overriding of preseptal orbicularis over pretarsal orbicularis • Lower lid retractor weakness which is recognized clinically by decreased excursion of the lower lid in downgaze.
Cicatricial entropion can effect either the upper and the lower lid. • Common causes include trachoma, acid and alkali burns and chronic conjunctival inflammations such as ocular pemphigoid.
Ectropion • Ectropion or the eversion of the lid margin can be congenital and acquired. • The acquired forms are the result of either ageing changes (involutional ectropion), or mechanical reasons (caused by tumors) or the scarring of the anterior lamella (cicatricial ectropion) or weakness of the orbicularis muscle (paralytic ectropion)
Ptosis: Abnormally low position (drooping) of the upper lid. • Neurogenic • Third nerve palsy • Horner syndrome • Marcus Gun jaw-winking syndrome • Third nerve misdirection
Ptosis • Myogenic • Myastenia gravis • Myotonic dystophy • Ocular myopathy • Simple congenital • Blepharophimosis syndrome
Ptosis • Mechanical • Aponuretic • Involutional • Postoperative
Blepharophimosis Syndrome:Telecanthus, epicanthus inversus,bilateral ptosis
Simple Congenital Ptosis • This is caused by a developmental dystrophy of the levator muscle. • It can be bilateral or unilateral • In down gaze the ptotic eye lid is slightly higher then the normal eye lid as a result of poor relaxation • Frequently there is absence of the upper eye lid crease • Usually levator function is poor • Sometimes weakness of the superior rectus muscle may accompany
Marcus Gunn Jaw-winking: A retraction of the ptotic lid in conjunction with stimulation of the ipsilateral pterygoid muscle
Third nerve misdirection: Bizarre movements of the upper lid which accompany various eye movements
Evaluation of the patient with ptosis • Margin-reflex distance : This is the distance between the upper lid margin and the light reflex in pupil is normally 4-4.5mm. If this distance decrases then there is ptosis.
Evaluation of the patient with ptosis • Vertical fissure height: This is the distance between upper and lower eye lids margins. Normally upper eye lid margin rests 2 mm below the upper limbus, and lower eye lid margin rests 1 mm above the lower limbus. VFH is 9mm in males and 11mm in females.
Evaluation of the patient with ptosis • Levator Function can be assesed by the upper the lid excursion. It is measured after eliminating frontalis muscle function by pressing above the eye brow and ask the patient to look down, and up. The amount of excursion is measured with a ruler. • Normal:15mm or more • Good: 12mm • Fair:5-11mm • Poor:4mm or less
Treatment of ptosis • Congenital ptosis in which levator function is poor, • Levator resection is the most chosen operation • Other procedures: Frontalis Brow Suspension
Treatment of ptosis • Involutional and aponeurotic ptosis: In this condition levator function is mostly good and the pathology is the detachment of the levator muscle from the upper border of the tarsus so we just attach the levator back to the upper tarsal border.
It is very common in elderly, The eye lids have baggy appearance with indistint lid creases. Treatment is blepharoplasty Dermatochalasis
This condition is suspected when the upper lid margin is above the superior limbus. It is most commonly seen in thyroid eye disease Lid Retraction
These are very common, Bilateral vertical skin folds that overhangs from the upper or lower lid towards the medial canthus. They may give rise to a pseudo-esotropia. Epicanthal folds
This is an uncommon condition. There is increased distance between the medial canthi as a result of abnormally long medial tendons. It should not be confused with hypertelorism in which there is wide separation of the orbits. Telecanthus
This is uncommon congenital partial or full-thickness eye lid defect. The upper lid coloboma is not associated with systemic anomalies The lower lid coloboma is frequently associated with systemic anomalies such as Treacher Collins Syn. Coloboma
Unilateral, red, raised lesion Most common during first year of life Resolves spontaneously by the age 4-7 Steroid injections can be given for vision threatening cases Strawberry Naevus(Capillary Haemangioma)
Pyogenic Granuloma Fast growing granulamatous hemangioma which is usually after surgery or trauma
Keratoacanthoma • Uncommon benign but rapidly growing tumour • Most common in immunsuppressive patients
Most common pre-malign skin lesion Solar (Actinic ) Kertosis
Basal Cell Carcinoma • Most comman human malignancy • 90% cases occur in head and neck, 10% of these involve eye lid. • Slow groving, locally invasive but non metastasizing
It accounts for 5-10 % of eye lid malignancies Potentially more aggressive tumour than BCC There are 3 main clinical types Plaque like Nodular Ulcerating Squamoous cell carcinoma