Download
1 / 22
220 likes | 435 Views
Infiltrating Basal Cell Carcinoma. Maysoon ALGain Dermatology Demonstrator KAAU. Case Presentation. CC: growth on right side of nose HPI: 81 yo HF who first noted growth on right side of nose “last December”, progressively growing. PMH: arthritis SH: ½ ppd smoker X 25 years

E N D
Infiltrating Basal Cell Carcinoma Maysoon ALGain Dermatology Demonstrator KAAU
Case Presentation • CC: growth on right side of nose • HPI: 81 yo HF who first noted growth on right side of nose “last December”, progressively growing. • PMH: arthritis • SH: ½ ppd smoker X 25 years • ROS: denies F/C, significant weight loss • FH: non-contributory
Physical Exam • General: AAO, VSS and good • VA: 20/80 OD, 20/50 OS • Pupils: 3mm OU, no APD • External: extensive ulcerative lesion from bridge of nose to RLL and R cheek, with almost complete destruction of RLL and nearly complete ptosis of RUL • IOP, CVF, DFE normal OS, unobtainable OD
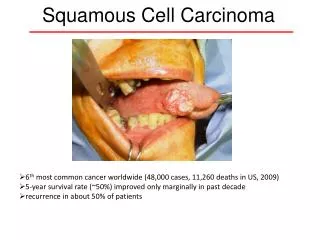
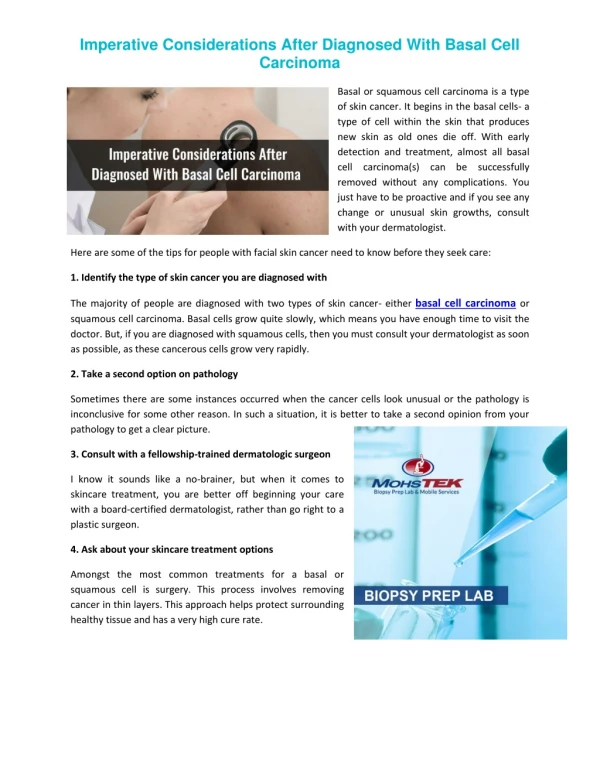
Differential Diagnosis • Malignant melanoma • Squamous cell carcinoma • Basal cell carcinoma, infiltrative • Infectious
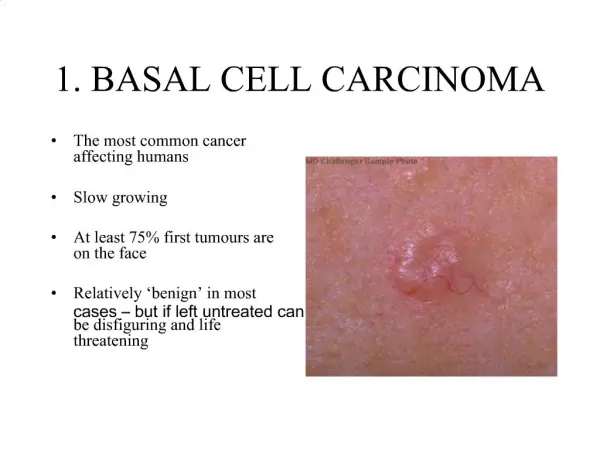
Basics of BCC • Background • Most common cutaneous malignancy (~80-90%) • Typically slow-growing, rarely metastasizes • Sun-exposed skin, mostly face and scalp, esp nose, cheek, and periorbital regions (~80%) • Frequency • 900,000 Dx in US/year • estimated lifetime risk of 33-39% for men and 23-28% for women • Sex • Men 2X over women
Basics of BCC • Mortality/Morbidity • <0.1% metastasize • Very low mortality • Significant morbidity with direct invasion of adjacent tissues, especially when on face or near an eye • Age • Likelihood increases with age • Rare in <40 yo • Race • Most often in light-skinned, rare in dark-skinned races
Superficial Nodular Micronodular Infiltrating (5%) Sclerosing/ morpheaform (5%) Metatypical Infundibulocystic Nodulocystic Adenoid Clear cell Follicular Sebaceous Perineurally invasive Variants of Basal Cell Carcinoma
Perineural Invasion • May be seen in 3% of pts with infiltrating and morpheaform types • Most often infiltrating type, which has highest rate of local recurrence • Requires CT scan for full work-up • Causes? inherently aggressive behavior vs inadequate early management?
Treatment Options • Electrodessication and curettage • Curettage alone • Surgical excision • Mohs micrographically controlled surgery • Cryosurgery • Ionizing radiation • Surgical excision plus radiation • Exenteration
Factors Considered in Treatment Planning • Pt preference to keep eye • Pt age • Surgical excision-considered definitive tx • “Careful frozen section controlled excision of periocular BCCs yields cure rates comparable to Mohs micrographic surgery at 5-year follow-up” • 5 year recurrence of 2.2% in one study • Wong, et al. “Management of Periocular Basal Cell Carcinoma with Modified En Face Frozen Section Controlled Excision.” Ophthalmic and Plastic Reconstructive Surgery. 2002. Vol 18 (6): 430-435. • Therefore, avoiding exenteration was considered a good possibility
Conclusion • Basal cell carcinomas are not always as innocent as we tend to believe • In formulating treatment course: • Strong pt preference and other pt factors • Current research