Download
1 / 25
250 likes | 327 Views
Which difference should we target?. Alberto Sobrero Ospedale San Martino IRCCS Genova, Italy. Which delta should we target?. Delta for deciding GO - NO GO to phase III ( signal generating trials) Delta of phase III. Randomized Phase II.

E N D
Which difference should we target? Alberto Sobrero Ospedale San Martino IRCCS Genova, Italy
Which delta should we target? • Delta for deciding GO - NO GO to phase III • (signalgenerating trials) • Delta of phase III
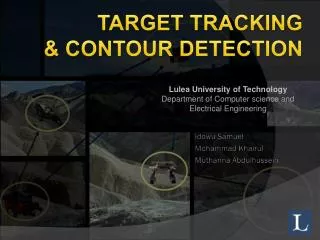
RandomizedPhase II Median PFS 6 vs 2.5 mo HR: 0.25 (0.1-0.5) Median OS 17.7 vs 6.7 mo HR 0.37 (0.2-0.7) Bendell JCO 2011
We expect too much from a Phase II • 1 Does the agent affect the naturalhx of the disease ? • Are we reasonably sure that the outcome would not have occurred in the absence of the investigational agent ? • 2 To whatextent? How sure are we of the size of the activity ? • 3 Isthiseffectenough to go to Ph III ? • Rationale. whyshouldit work in thisdisease ? • empirical, preclinicalevidence • PK-PD. Isoptimal dose and schedule defined ?
NO NO NO NO NO PFS on study vs PFS on prior regimens
Which delta should we target? • Delta for deciding GO - NO GO to phase III • (signalgenerating trials) • It is crucial that efficacy data from phase I-II whether comparative or non comparative be interpreted in the strictest way.
Size of benefit (target delta) : a compromise • plausible to achieve • worthwhile if achieved
Target delta: HR • 0.5 meansdoubling of the benefit vs control • 48 months • 0.66 means 50% increment of the benefit vs control • 46 months • 0.80 means 25% increment of the benefit vs control 45 months fantastic very good hmm…
15 pivotal R phase III registration trials, 9 biologics , 8 cancer types median HR PFS .57 OS .73 median absolute gain 2.7 months 2.0 months …hmm… Very good / fantastic Sobrero and Bruzzi , JCO 2009
The 3 problems HR vs absolute delta target HR in trial design vs p value in trial analysis and interpretation. low target HR in trial design
PROBLEM 1: ABSOLUTE GAIN Increase in median OS for different HR as a function of prognosis MST Increase in median values as a function of HR In control 0.9 0.8 0.7 0.6 0.5 0.4 6 .6 1.5 2 4 69 Clinically worthwhile relative delta is a function of prognosis Both HR AND absolute gain must be considered 24 2.6 6 10 16 24 36 worthless worthwhile Unrealistic
PROBLEM 2: INCONSISTENCY DESIGN CONDUCT ANALYSIS REPORT INTERPRET. Define target delta…………....target delta is ignored and... p value becomes the focus…
Problem 3 : INCONSISTENCY H1 H0 NEG POS POS POSITIVE HR 0.4 0.5 0.6 0.7 0.8 0.9 1.0
‘Statistically positive’ trials with deltas lower than those pre-specified in the protocol AUTHOR DRUG TUMOR predefined reported p HR HR value Johnstone 09 lapatinib breast 0.64 0.71 0.019 Jonker 07 cetuximab colon 0.74 0.77 0.001 Moore 07 erlotinib pancreas 0.75 0.82 0.038 Llovet 08 sorafenib liver 0.6 0.69 0.001 Escudier 07 sorafenib renal 0.67 0.72 0.02 modified from Ocana A. JNCI,2011
PROBLEM 3. ‘ LOW PROFILE’Typical phase III trial design in advanced cancer (PFS 6 mo) • Delta 25% i.e. HR = .75 • Median delta = 1.8 mo • Power 90% • N = 800 • Cost = 100 M If we get this , is this really clinically worthwhile? Be more corageous : raise the bar
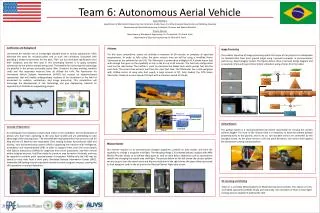
TML OS: ITT population 1.0 CT (n=410) BEV + CT (n=409) 0.8 Unstratifieda HR: 0.81 (95% CI: 0.69–0.94) p=0.0062 (log-rank test) 0.6 Stratifiedb HR: 0.83 (95% CI: 0.71–0.97) p=0.0211 (log-rank test) 0.4 OS estimate 0.2 0 9.8 mo 11.2 mo 0 6 12 18 24 30 36 42 48 Time (months) No. at risk CT 410 293 162 51 24 7 3 2 0 BEV + CT 409 328 188 64 29 13 4 1 0 Median follow-up: CT, 9.6 months (range 0–45.5); BEV + CT, 11.1 months (range 0.3–44.0) aPrimary analysis method; bStratified by first-line CT (oxaliplatin-based, irinotecan-based), first-line PFS (≤9 months, >9 months), time from last dose of BEV (≤42 days, >42 days), ECOG performance status at baseline (0, ≥1)
VELOUR Overall Survival - ITT Population Cut-off date = February 7, 2011; Median follow-up = 22.28 months
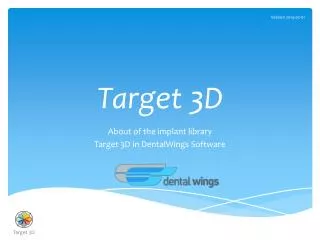
CORRECT Overall survival • Regorafenib Placebo 1.00 Median 6.4 mos 5.0 mos 95% CI 5.9–7.3 4.4–5.8 0.75 Hazard ratio: 0.77(95% CI: 0.64–0.94) 1-sided p-value: 0.0052 Survival distribution function 0.50 0.25 Placebo N=255 Regorafenib N=505 0 0 50 100 150 200 250 300 350 400 450 Days from randomization Primary endpoint met prespecified stopping criteria at interim analysis (1-sided p<0.009279 at approximately 74% of events required for final analysis)
The different aspects of clinical benefit • HR • Median • % at prespecified time • % cure/ long term survivors • Clinically meaningful responses • Toxicity and logistical convenience
Conclusions • ‘critical’ HR of around 0.75 is appropriate for most conditions • Primary endpoint depends on setting • All other parameters of efficacy and toxicity must be evaluated to correctly interpret the clinical relevance of ‘incrementalist’ delta.