Neonatal Apnea: Causes, Diagnosis, and Care
580 likes | 704 Views
Learn about neonatal apnea, including causes, diagnosis, and care for infants experiencing breathing pauses. Understand the potential causes and consequences of apnea, as well as the methods for evaluating and managing this condition.

Neonatal Apnea: Causes, Diagnosis, and Care
E N D
Presentation Transcript
Neonatal Apnea M.Noori-Shadkam, MD-MPH Neonatologist
Periodic Breathing • Recurrent sequences of pauses in respiration lasting for 5-10 seconds and followed by 10-15 seconds of rapid respiration.
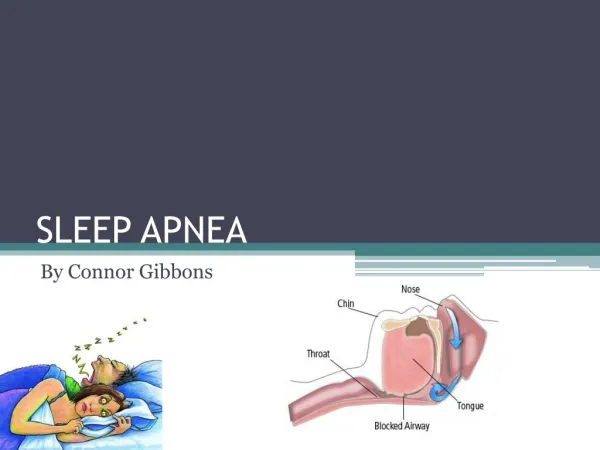
DEFINITION Apnea is defined as the Cessation of airflow for at least 20 seconds or a shorter respiratory associated with bradycardia or cyanosis. Bradycardia and cyanosis are usually present after 20 sec. of apnea. After 30 to 45 sec., pallor and hypotonia are seen, and infant may be unresponsive to tactile stimulation.
Incidence • The incidence of apnea in term infant is quite low. As a result, the cause of apnea in term infant should to be pathologic. • In a multicenter study, apnea was diagnosed in 50 percent of infant born between 33-34 weeks gestations. • Apnea occurs in virtually all infants born at less than 28 weeks gestation.
Incidence • In term infants, apnea is always worrisome and demands prompt diagnostic evaluation. As a result, the cause of apnea in term infant should to be phathologic.
Potential causes of Neonatal Apnea and Bradycardia .Centeral nervous system IVH Seizure (along with fluttering eyelids, drooling or sucking, tonic posturing) Hypoxic Injury . Respiratory Pneumonia Obstructive airway lesions
Potential causes of Neonatal Apnea and Bradycardia Upper airway collapse Atelectasis Extreme Prematurity Laryngeal reflex Phrenic nerve paralysis Pneumothorax Aspiration
Potential causes of Neonatal Apnea and Bradycardia .Infections Sepsis Meningits(bacterial, viral&fungal) Rsv Pertusis
Potential causes of Neonatal Apnea and Bradycardia .Gasterointestinal Overdistention of stomach GER with or without aspiration(due to laryngospasm, stimulation fo irritant receptors in lower esophagous) NEC
Potential causes of Neonatal Apnea and Bradycardia Metabolic Gloucos Sodium Amonia Organic acids Alkalosis
Potential causes of Neonatal Apnea and Bradycardia cardiovascular hypotention Hypertention Heart failure Hypovolemia Vagal tone PDA & CHD
Potential causes of Neonatal Apnea and Bradycardia .Other Anemia( oxygen carring capacity of blood& Arterial pressure perfusing CNS) Polycythemia ( blood viscosity and blood flow to CNS) Hypothermia hyperthermia
Potential causes of Neonatal Apnea and Bradycardia Immaturity of respiratory center Sleep state Pain Antepartum administration of my sou or opiates to the mother Administration of opiates or general anesthesia to the infant
.These disorders produce apnea by direct depression of the centeral nervous system’s control of respiration. Hypoglycemia Meningitis Drugs Hemorrhage Seizure
Disturbances in oxygen delivary shock Sepsis anemia
Potential causes of Neonatal Apnea and Bradycardia Ventilation defect Obstraction of the airway pneumonia Muscle weakness
PREMATURITY Impaired Inhibitory Oxygenation Reflexes APNEA Infection CNS pathology Metabolic disorders Specific causes of apnea
Apnea of prematurity . Apnea of prematurity is a developmental disorder that reflects physiologic rathar than pathologic immaturity of respiratory control. • In preterm infants, the Immaturity of breathing responses affects all levels of respiratory control, Including central and peripheral chemosensitivity and inhibitory pulmonary neuronal.
Apnea of prematurity Preterm infants respond to a fall in inspired oxygen with a transient hyperventilation followed by hypoventilation and sometimes apnea.
Types of Neonatal Apnea • Central (diaphragmatic) • Peripheral (obstructive) • Mixed
Consequences of Apnea Gas exchange is compromised due to: • PA CO2, PAO2 • Extrapulmonary shunting • Muscle relaxation
Evaluation of determinecause of apnea .The goal of the diagnostic evaluation is to differential apnea of prematurity from other causes of neonatal apnea . Maternal administration of my sou or opioids .Neonatal administration of opioid.
Evaluation of determine cause of apnea • Risk factor for neonatal sepsis • Traumatic delivery and/or perinatal asphyxia • Sign and symptoms of hypoglycemia • Sign and symptoms of sepsis • Sign and symptoms fo IVH • Assessment of the airway to detect congenital anomalies of the upper airway
Evaluation of determine cause of apnea .Sign and symptoms of NEC .Laboratory evaluation Includes:CBC,BC,BS,ABG, .Cranial imaging
Care fo the infant 1.BP should be measured frequently and hypotension with oliguria< 2 mL/kg/h should be treated accordingly 2.Hct should be> 45% ???
Care of The Infant 3.Prevent hyperflexion of the neck 4.Nurse the baby in prone position 5.Set the thermal environment to obtain a central temperature of 36.5-37⁰ C 6.Minimize the duration and rate of pharyngeal suction cont’d
Care of The Infant 7. Place the orogastric tube carefully 8. Avoid sudden gastric distension 9. Continuous gastric feeding if apnea occurs with gavage 10. Warm air and oxygen to incubator temperature
Nursing Management During Apneic Episode • Check infant at once • Cancel alarm • Stimulate if there is no obvious vomit • Suction cont’d
Nursing Management During Apneic Episode 5. Give O2 via face mask in same concentration as infant had been receiving 6. Summon help if infant does not respond 7. Document and report 8. Intubation if indicated
Management of Idiopathic Apnea • When apneic spells are repeated and prolonged, (i.e., more than 2 to 3 times/h.) or when they require frequent bag and mask ventilation, treatment should be initiated. cont’d
Management of Idiopathic Apnea • Diagnosis and treatment of specific causes • Nursing care • Nasal CPAP (4-6 cm H2O) • Methylxanthine therapy • Increased environmental O2 only as necessary to maintain adequate baseline O2 saturation. Often associated with treatment of anemia • Assisted ventilation if all else fails
Management of Idiopathic Apnea • General measures 1. Diagnosis and treatment of specific causes 2. SO2 : 85-95% 3. Avoid reflexes that may trigger apnea. Suctioning of the pharynx should be done carefully, and oral feeding should be avoided. cont’d
Management of Idiopathic Apnea 4. Position of extreme flexion or extension of the neck should be avoided, to reduce the likelihood of airway obstruction. 5. Avoid swings in environmental temperature. cont’d
Management of Idiopathic Apnea 6. Consider a transfusions of PRBCs if the Hct is <25% and the infant has episodes of apnea and bradycardia that are frequent or severe while methylxanthine levels are therapeutic. cont’d
Management of Idiopathic Apnea B. Nasal CPAP (4-6 cm H2O) can reduce the number of mixed and obstructive apneic spells. C. Methylxanthine (caffeine of theophylline) therapy, commencing with a loading dose followed by maintenance therapy, and serum level monitoring, especially for theophylline. D. Assisted ventilation if all else fails
Monitoring • Because impedance apnea monitors may not distinguish respiratory efforts during airway obstruction from normal breaths, heart rate should be monitored in addition to, or instead of, respiration.
Monitoring • All preterm infants below 35 WG must be monitored for at least the first week after birth. Monitoring should continue until no significant apneic episode has been detected for at least 5 days.
CPAP Effects • PaO2 with increased lung volume & C • Work of breathing • Splitting of the upper airways • Elimination of the intercostal inspiratory- inhibitory reflex
Pharmacologic Mechanisms for Methylxanthine • Competitive effect on adenosine receptors • Sensitivity of respiratory center to CO2 • Afferent nerve traffic to brain stem • Catecholamine response • Central stimulation (inspiratory drive) • Improved skeletal muscle contraction • Improved metabolic homeostasis • Improved oxygenation via increased cardiac output and decreased hypoxic episodes
Signs of Toxicity in Infants Receiving Theophylline • Failure to gain weight 10-20 µg/mL • Sleeplessness • Irritability • Tachycardia • Hyperglycemia • Vomiting 20 µg/mL • Diuresis/dehydration • Jitteriness > 20 µg/mL • Hyperreflexia • Cardiac arrhythmias > 40 µg/mL • Seizures
prognosis apnea of prematurity doesnot after an infant’s prognosis unless in is severe, recurrent, and refractory to therapy. apnea of premuturity usually resolves by 37 wk or postconceptional ages although it may persist beond term gestatoin.
prognosis apnea of permaturityisnot a risk factor for SIDS. Some infant with persistent apnea are discharges with cardio respiratory monitoring performed at home.
prognosis In the absence of significant events, Home monitoring can be safely discontinued after 44 wk post conceptional age. What time dose begin treatment?
prognosis Episodes at apnea ˃10 episodes in 24h No respond to skine actuation Need to bag and mask
Anemia Transfusion in HCT≤25 An increase in episodes of apnea and bradycardia (˃ episodes in a 24hr or ≥ 2 episodes in 24hr requirng bag and mask ventilation ) while. Infant is riceiving therapeutic does of methylxanthines.
Side effect of Donapam: Irritability hypoylycemia gastric irritation Secod-degree heart block An overnight polysomnographic study in the most complete test for evaluation of infant apnea.