Download
1 / 20
340 likes | 911 Views
Acetylcholinesterase Inhibitors in the Treatment of Alzheimer’s and Dementia. Pharmaceutical Chemistry II – SSPPS 222 Based on Presentation from : Victor Ramos, Lisa Ferris, and Sarah Brown. Disease : Alzheimer’s Disease & Stats. Alzheimer’s is a form of dementia 2012 Statistics

E N D
Acetylcholinesterase Inhibitors in the Treatment of Alzheimer’s and Dementia Pharmaceutical Chemistry II – SSPPS 222 Based on Presentation from : Victor Ramos, Lisa Ferris, and Sarah Brown
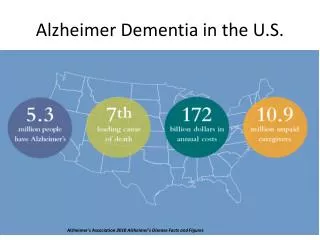
Disease: Alzheimer’s Disease & Stats Alzheimer’s is a form of dementia 2012 Statistics • 5.4 million citizens (5.2 million 65 and older) • One in eight older Americans • By 2025, 6.7 million (30% increase) • 2/3 of Alzheimer’s sufferers are women • 6th leading cause of death in the United States • Payments for care are estimated to exceed $200 billion • 80% of care is delivered by family (valued at over $210 billion) http://www.alz.org/downloads/facts_figures_2012.pdf
Disease: Some Alzheimer’s Etiologies and Possible Therapeutic pathways Degradation of Acetylcholine
Disease/Drugs: History of AZ Drugs for Different Pathways • Acetylcholinesterase inhibitors • 1993: Tacrine approved for mild to moderate Alzheimer’s symptoms • 1996: Donepezil approved for mild to severe Alzheimer’s symptoms • 2000: Rivastigmine approved for mild to moderate Alzheimer’s symptoms • 2001: Galantamineapproved for mild to moderate Alzheimer’s symptoms • Namenda (NMDA receptor antagonist) • 2003: Namenda approved for moderate to severe Alzheimer’s symptoms • 2010: Namenda XR approved for moderate to severe Alzheimer’s symptoms
Target 1: AChE: Mechanism of Action • Acetylcholinesterase breaks down Ach into choline and an acetate through hydrolysis • Acetylcholinesterase inhibitors block this reaction in several regions of the brain • There is a significant correlation between acetylcholinesterase inhibition and observed cognitive improvement
Target: Acetylcholinesterase • 2 general classes of molecular forms • Simple homomericoligomers of catalytic subunits • Founds as soluble species in cell • Exported • Heteromeric associations of catalytic subunits with structural subunits • Found in neuronal synapses • Tetramer of catalytic subunits disulfide linked to a 20kDa lipid-linked subunit • Outer surface of cell membrane
Target: Acetylcholinesterase • Acetylcholinesterase rapidly hydrolyzes Ach • Terminates transmission at cholinergic synapses • Alzheimer’s may involve depletion of Ach • Inhibition of acetylcholinesterase could help symptoms • Active Site • Esteraticsubsite: catalytic machinery • Anionic subsite: binds quaternary group of Ach • Peripheral anionic subsite: 14Å from anionic subsite • Enhanced potency if drug can span both active sites
Target: Acetylcholinesterase Site • Contains catalytic triad • Located at bottom of aromatic gorge • Deep, narrow cavity • 40% lined by rings of 14 aromatic amino acids • Primary site of interaction between quaternary group of Ach and acetylcholinesterase is aromatic ring of Trp-84 • Trp-84 and Phe-330 part of anionic subsite • Trp-275 part of peripheral anionic subsite
Drug Molecules Tacrine Donepezil Galantamine • Tacrine has no chiral centers • Galantamine has three chiral centers and the (S,R,S) conformer is the naturally occurring form • Donepezil’s two stereoisomers show activity but its R-enantiomer has more activity
Drug: Tacrine • Normally, phenyl ring of Phe-330 lies parallel to surface of gorge • When tacrine binds, it makes contact with the bound ligand • Ring of Phe-330 is rotated about both X1 and X2 • Tacrine is thus sandwiched between between the rings of Phe-330 and Trp-84 • Recall Trp-84 is primary site of interaction between Ach and acetylcholinesterase
Drug Groups: Donepezil • Three segments of Donepezil, all interact with Acetylcholinesterase gorge • Dimethoxyindanone • Inandone ring has pi-pi interactions with indole ring of Trp279 • Piperidine • Cation-pi interaction with Phe330 • Ring N makes H bonds with water which makes H bonds with Tyr121 • Benzyl • Parallel π–π stacking with the Trp84 indole, • Makes an aromatic H-bonds with water molecules that H-bond to the residues of the oxyanion hole, namely with Gly118 N, Gly119, Gly201 N, and Ser200 • Occupies the binding site for quaternary ligands such a ACh
Drug Groups: Galantamine • The inhibitor spans the active site gorge, including the acyl binding site • Hydrogen bonding • Two H-bonds form between the hydroxyl of the inhibitor and Glu-199 and Ser-200 and the inhibitor’s oxygen molecule • Water molecules • Rest of interactions are Non-Polar • Notable that galantamine lacks the characteristic cation-pi interaction with Phe-330 • Pi-stacking occurs between the double bonds in the cyclohexene ring of GAL and the indole ring of Trp-84 • No charge-charge interactions
Drugs: Side Effects • Tacrine • Causes elevated hepatic enzymes (CYP1A2) and is hepatotoxic • Tacrine metabolite is cytotoxic • Off market • Galantamine • Abdominal pain, diarrhea, nausea related to cholinergic effects • Resolve with continued treatment • Donepezil • Well tolerated at 5 mg/day • 13% discontinuation rate at 10 mg/day. • Gastrointestinal side effects are most common, related to cholinergic effects • All acetylcholinesterase inhibitors act through similar mechanisms, so GI side effects are similar, with severity depending on the dose administered • Increased acetylcholine over-stimulates cholinergic receptors in the GI tract to cause secretory and motor activity
Drug-Drug Interactions • CYP34A inhibitors like erythromycin, cimetidine, and saquinavir increase bioavailability of the drugs and lead to increased adverse effects • The same is true for CYP2D6 and CYP1A2 inhibitors • In contrast, inducers of these metabolic enzymes like phenytoin and rifampicin will decrease bioavailability and lead to limited efficacy of the drugs
Future Treatments • Immunizations that utilize the immune system to attack beta-amyloid plaques • This went to clinical trials but was stopped when some participants developed acute brain inflammation • Anti-amyloid antibodies derived from other sources infused into the blood via IV • Preventing neurofibrillary tangles • Reducing chronic neuron inflammation associated with Alzheimer’s • NSAIDs have had variable effects
Conclusion • These drugs effectively inhibit acetylcholinesterase from hydrolyzing acetylcholine into choline and an acetyl group • However, this may or may not be effective in prolonging onset or reducing symptom severity in Alzheimer’s and does not address the underlying pathophysiology of the disease state • New treatments will likely target other factors involved in Alzheimer’s – drugs targeting amyloid-beta plaques and tau proteins are currently being developed • Combination therapies
References "2012 Alzheimer's Disease Facts and Figures." Alzheimer's and Dementia 8.2 (2012): 1-67. 2012. Web. 7 Mar. 2013. A. Koster, Hemmung der cholinesterasen in verscheidenenorganendurcheserin, galanthamine und tacrin; conzentrations-wirkungsbeziehungen, bedeuting fir die therapeutischanwendung. Dissertation 1994; MedezinsicheFakultat der Humboldt Univzu Berlin. Abagyan, R.,Physical Pharmacology. http://xablab.ucsd.edu/ (accessed March 5, 2013). "Alzheimer's Disease Treatments." Alzheimer's Disease Treatments. BrightFocus Foundation, 4 Oct. 2012. Web. 07 Mar. 2013. "Alzheimer's Treatments: What's on the Horizon?" Mayo Clinic. Mayo Foundation for Medical Education and Research, 06 Mar. 2013. Web. 07 Mar. 2013. "Drug Bank: Donepezil." DrugBank. GenomeQuest, 8 Feb. 2013. Web. 7 Mar. 2013. "Drug Bank: Galantamine." DrugBank. GenomeQuest, 8 Feb. 2013. Web. 7 Mar. 2013. "Drug Bank: Tacrine." DrugBank. GenomeQuest, 8 Feb. 2013. Web. 7 Mar. 2013. Greenblatt, H., et al. "Structure of AcetylcholinesteraseComplexed with (-)-galanthamine at 2.3 A Resolution." Federation of European Biochemical Societies 463 (1999): 321-26. FEBS Letters, 8 Nov. 1999. Web. 7 Mar. 2013. Harel, M., et al. "Quaternary Ligand Binding to Aromatic Residues in the Active-site Gorge of Acetylcholinesterase." ProcNatlAcadSci U S A 90.19 (1993): 9031-035. PubMed. Web. 7 Mar. 2013. Kryger, G., et al. "Structure of AcetylcholinesteraseComplexed with E2020 (Aricept®): Implications for the Design of New Anti-Alzheimer Drugs." Structure 7.3 (1999): 297-307. Elsevier Science Ltd., 1 Mar. 1999. Web. 7 Mar. 2013. Maccioni, R., Perry, G., Current Hypotheses and Research Milestones in Alzheimer's Disease. New York: Springer, 2009. Print. Massouli, J Molecular forms and anchoring of acetylcholinesterase. In, Cholinesterases and Cholinesterase Inhibitors. (Giacobini E, ed) Martin Dunitz, London, 2000 pp. 81-103 Sussman, J.. et al. "Atomic Structure of Acetylcholinesterase from Torpedo Californica: A Prototypic Acetylcholine-Binding Protein." Science 253 (1991): 253-61. Sciencemag.org. 21 Dec. 2006. Web. 7 Mar. 2013.