Primitive reflexes
Primitive reflexes explained well by Dr. Miloni Shah<br><br>Also access my videos for primitive reflexes on YouTube<br>click on the link below<br>https://www.youtube.com/playlist?list=PLhpSymrcaX-R_0shZ4M8sQ4drv5xuBveg<br><br>#, #, #, #, #, #, #, #pediatricphysicaltherapist, #medschool, #physiomom, , #physio, #physiomommy, #y, #<br><br>

Primitive reflexes
E N D
Presentation Transcript
Primitive Reflexes By: Dr. Miloni Shah Guided: Dr. Rima jani
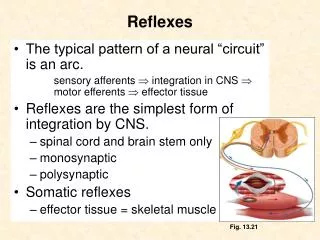
Contents: • Introduction • Reflex arc • Classification of reflexes • Significance of reflexes • Types of reflexes
Introduction • A reflex is an involuntary or automatic, action that your body does in response to something without you even having to think about it. • Neonatal reflexs are inborn reflex which are present at birth and occur in a predictable fashion. A normally developing newborn should respond to certain stimuli with these reflexes, which eventually become inhibited as the child matures. • These reflexes are then replaced by voluntary motor skills. • When the reflexes are not inhibited, there is usually a neurological problem at hand.
Classification Depending upon their situation of the center Depending upon whether inborn or acquired Depending upon their function
Types • Automatic reflexes • Spinal reflexes • Brain stem reflexes • Midbrain reflexes • Cortical reflexes
Automatic reflex • Moro reflex • Gallants trunk reflex • Parachute reflex • Landau reflex
Moro reflex (startle reflex)protective” response” • An involuntary protective motor response against abrupt disruption of body balance or extremely sudden stimulation. • This reflex is also related to a baby’s development of head control • TESTING POSITION: child is in halfway position between supine and upright position • STIMULUS: loud noise, bright light, or even a sudden movement that the infant produces themselves or support is withdrawn from the head • RESPONSE: There will be shoulder abduction and elbow wrist and finger extension followed by shoulder adduction and elbow wrist and finger flexion • ONSET :birth • INTEGRATED: 6 months
Retained moro reflex • Mood swings/sudden changes in behavior • Anxiety • Visual challenges • Learning difficulties • Depression • ADHD • Autism • Emotional and social immaturity • Coordination and balance challenges • Poor tolerance to change • Dyslexia and/or Dyscalculia
Integration • Visual challenges: • More ball games to promote visual tracking skills. Instead of throwing and catching, try something simpler such as rolling a tennis ball back and forth across the table. • Reading with a highlighter strip or a piece of paper under the line that is being read. This helps the eyes focus on the line and decreases distracting visual input. • Learning difficulties, Dyslexia, and Dyscalculia: • Talk with your child’s teacher about strategies in the classroom and accommodations that can be provided.
Anxiety: • Try calming activities such as deep pressure and heavy work (proprioceptive input) - weighted blanket, massage, movements that work the muscles such as pushing/pulling, animal walks, etc. • Visual schedules - this can help the child understand time and space and know when certain things will be happening. • Noise-cancelling headphones - if your child is sensitive to sound, this can cause anxiety with certain situations. Try noise-cancelling headphones to decrease the auditory input. • Therapeutic Listening Programs • Coordination and balance challenges as well as motion sickness: • Incorporate more movement into the day. • Try obstacle courses, playing on playground equipment, jumping and crashing, balance games, etc.
Parachute reflex • TESTING POSITION: vertical position • STIMULUS: Infant is held in prone in the air and then suddenly thrust head fist towards the examining table or floor • RESPONSE: infant will immediately extend and abduct slightly and the fingers spread as if attempt to break the fall. • ONSET :5-9 months • PRESENT: through out life
Abnormality in this reflex • Absent or abnormal in children with cerebral palsy and severe motor disorders. • Asymmetry in this indicates upper extremity weakness or spasticity • This reflex doesn’t require vision so can be done blindfolded
Gallants trunk reflex • TESTING POSITION: prone position • STIMULUS:There will be stroking or tapping on one side of the infant spine • RESPONSE: there will be side flexion on the side which is stroked and hips are also raised towards that side • ONSET :birth (20 weeks of in utero) • INTEGRATED 3-9 months of age • The Spinal Galant is believed to play an important role in the natural birthing process.
Retained gallants trunk reflex • Delay in preparation of crawling and walking • Problem in urination so bed wetting problem occurs • Tactile hypersensitive • Gait can be affected which can lead to limp contributing to scolosis • Inability to sit still, • short-term memory loss or an inability to concentrate. • Fidgeting is present • Prevelance of ADHD
Integration • Snow angels • Vibration,Wilbarger Brushing Protocol for hypersensitive to tactile & for fidgeting • Proprioceptive input is calming to the nervous system, so complete 5-10 minutes of heavy work activities prior to sitting down for a focused task • Try compression clothing - instead of having a shirt or pants that “tickle” the back and stimulate the reflex, try tight compression clothing that won’t rub or move. • Bedwetting • Decrease the amount of liquids before bed. • Change what your child sleeps in, attempting to decrease clothing that moves against the back
Landau reflex • TESTING POSITION: supporting the infant horizontally in air in prone position • STIMULUS: passive flexion or extension of the head • RESPONSE: if flexion hip knee and spine also flexed and elbow • If extension of head ,extension of spine hip knee and elbow • ONSET: 3 months • INTEGRATED: 3 years
Retained landau reflex • Low muscle tone • Poor posture • Poor motor development • Short term memory difficulty • Weak upper body • Attention and concentration problem • Toe walking
Integration • Deep pressure • Proprioception activities • Weight bearing activities • swinging pushing and pulling activity
Spinal cord reflex • Rooting reflex • Sucking reflex • Palmer reflex • Planter reflex • Flexor withdrawal reflex • Extensor withdrawal reflex • Cross extensor withdrawal reflex • Stepping reflex • Babinski reflex • Babinski reflex
Spinal cord reflex • Rooting reflex • Sucking reflex • Palmer reflex • Planter reflex • Flexor withdrawal reflex • Extensor withdrawal reflex • Cross extensor withdrawal reflex • Stepping reflex • Babinski reflex • Babski reflex
Rooting reflex (search reflex) • TESTING POSITION: supine lying • STIMULUS:initiates when the corner of an infant’s mouth is stimulated by stroking • RESPONSE:the newborn will turn his or her head towards the stimulus and open the mouth with tongue thrusting. • ONSET: birth • INTEGRATED: 4months • This is replaced by voluntary sucking as the child grows
Sucking reflex • TESTING POSITION: supine lying • STIMULUS:initiates when roof of an infant’s mouth is touche the nipple or finger • RESPONSE: infant will automatically start sucking the nipple or finger • ONSET: birth( 32 weeks of pregnancy ) • INTEGRATED: 4months
Retained rooting and sucking reflex • Tongue lies too far forward • Hypersensitive around the mouth • Thumb sucking can remain • Speech and articulation problems • Difficulty in swallowing and chewing • Dribbling • Difficulty with texture and solid foods
Palmar grasp reflex • TESTING POSITION: supine lying • STIMULUS:examiner inserts his or her finger into the palm of the infant from the ulnar side and applies pressure to the palm • RESPONSE: fingers closing around the object that provided pressure, as well as gripping or holding on • ONSET: birth( 11 weeks IU) • INTEGRATED: 3 months
Retained palmar grasp • Challenges with fine motor tasks, including grasp on small objects, handwriting, self-feeding, and manipulation of clothing fasteners • Potential challenges with speech and articulation • Overflow into the mouth during fine motor tasks (sticking tongue out, etc.) • Tactile hypersensitivity - specifically to hands • Challenges with directionality (left vs right) • Dysgraphia • Voluntary grasp and release is not possible
Plantar grasp reflex • TESTING POSITION: supine lying • STIMULUS:By pressing a thumb against the sole of the foot just behind the toes • RESPONSE: It consists of the flexion and adduction of all toes as if the toes were firmly grasping the stimulating object[ • ONSET: birth (32 weeks UI) • INTEGRATED: 9 months
Retained plantar grasp • Normal walking is not present • Disturbance in gait • balance affection occurs • Toe walking may be present
Flexor withdrawal reflex) (protective reflex) • TESTING POSITION: supine lying head in neutral and legs extended • STIMULUS: sole of the foot is stroked • RESPONSE: there will be flexion of the stimulated foot • ONSET: birth(28 weeks of gestation) • INTEGRATED: 1-2 months
Extensor withdrawal reflex • TESTING POSITION: supine lying head in neutral and legs extended • STIMULUS: sole of flexed foot is stroked • RESPONSE: there will be extension adduction internal rotation of the flexed leg with planter flexion of the foot • ONSET: birth • INTEGRATED: 4 months
Retained reflex • Tactile defensive behaviour • Abnormality in gait • Intergration • Joint compression • Give maximum weight bearing position
Crossed extensor withdrawal • TESTING POSITION: supine lying head in neutral and legs extended • STIMULUS: noxious stimulus to the ball of the foot • RESPONSE: opposite lower limb flexes ,then adducts and extends • ONSET: birth(28 weeks of gestation) • INTEGRATED: 1-2 months
Retained reflex • Difficulty in walking • Poor posture • Balance maintenance will be difficulty • Develop hip adductor tightness( scissoring gait)
Intergration • Butterfly sitting position • Joint compressions • Calipers might be needed is gait abnormality are severe because of muscle imbalance
Stepping reflex • TESTING POSITION: baby is hold upright • STIMULUS: when sole of the foot touches the couch • RESPONSE: leg lift and will try to decent • ONSET: birth • INTEGRATED: 6 months • Retained stepping reflex • Premature will try to walk in a toe heel fashion of walking
Babinski reflex • TESTING POSITION: supine lying • STIMULUS: when sole of the foot is stimulated with blunt instrument • RESPONSE: extension of the great toe and fanning of other toes • ONSET: birth • INTEGRATED: 12-24 months • Retained Babinski sign indicative of upper motor neuron lesion contributing damage of the corticospinal tract.
Babski reflex • STARTING POSITION: supine lying • STIMULUS: deep pressure applied simultaneously to the palm of both hands • RESPONSE: flexion or forward bowing of the head ,opening of the mouth and closing of eyes. • ONSET: birth • INTEGRATED: 4 months • Retained reflex-there will be problem with have chance of cerebral palsy and mental retardation.
Brainstem reflex • Aysmterical tonic neck reflex • Symetical tonic neck reflex • Tonic labrythine neck reflex • Positive supporting reflex • Negative supporting reflex
ATNR (Fencer’s pose) • TESTING POSITION: supine lying position • STIMULUS: Turing of head to any one side (rt) side • RESPONSE: Flexion of arm and leg on the skull side • Extension of arm and leg on the face side • ONSET: birth • Integrated : till 6 months of age
Retained ATNR • Because the ATNR is directly related to the vestibular system and consists of a physical reaction, it has a direct impact on movement, balance, muscle tone, and coordination. Additionally, due to the movement of the arm in relation to the head, it also has a direct impact on hand-eye coordination. • Challenges with crawling as an infant • Decreased engagement with toys as an infant • Poor balance when learning to walk • Gravitational insecurity and fear with movement • Challenges crossing midline • Poor hand dominance establishment • Challenges with reading and writing • Left / right confusion • Challenges with visual tracking • Poor coordination for bilateral integration tasks • Dyslexia and/or Dysgraphia
INTEGRATION • If your child is young, under three months old, • Proper tummy time, place toys to the left and the right side, not just in front. Use noise and gentle lights to engage the visual system and encourage head turns to look at objects. • Encourage more crawling activities. Use pop up tunnels, create tunnels using chairs and blankets, etc. Try to engage the child visually to facilitate head turns while they are crawling. • Facilitate crawling across a variety of floor textures and thresholds.
If your child is older, you can still focus on the same developmental movements and increase the challenges, as well as try some other activities. • Set up a matching game on the floor - place colored pieces of paper on the floor in a semi-circle around the child, who will lay on their stomach. Call out a color and have the child reach to tap the color. Encourage crossing midline - reaching with left hand to tap a color on the right, and vice versa. • Slow swinging tasks ,simple balance activities with balance beams, hopping on one foot, etc. Try balancing on one foot with eyes closed - time it and try to beat your time. • Simply bouncing and rolling activities with therapy ball - give them control over the movement to feel safer. • Jumping jacks, cross crawl, , and Obstacle courses are useful.
STNR • TESTING POSITION: Quadripod • STIMULUS: when there neck extension/neck flexion • RESPONSE: arms will straighten while the legs will flex / arms will flex while the legs will straighten - moving the infant into a somewhat down dog position. • ONSET :6-8 months • INTEGRATED: 12 months of age
Retained STNR • Minimal to no crawling • Poor posture • W-sitting • Lays head on desk during focus tasks • Decreased hand-eye coordination • Challenges with near-far point tracking • May seem clumsy, poor overall coordination • May be a messy eater • Challenges with attention and focus • Challenges with reading and writing • Difficulty copying from the board • Signs of Dyslexia
INTEGRATION • Get them crawling • Use tunnels to facilitate crawling. Roll balls and push toys through, have motivating toys on the other side, etc. Make your own by placing a blanket over 2 or more objects. • Cat-Cow movement , Jumping jacks • Prone reach outs • Creeping and crawling • Midline crossing activities • Use therapy ball to activate the core muscles to decrease a slouched position. • Provide more rest breaks during physical activity. Poor posture is often accompanied by fatigue. • During mealtime, use a mirror to bring attention to what the hands and mouth are doing, notice where food is, etc.
Tonic labrynthine reflex(superman pose) • This reflex is activated with neck flexion (forward) or extension (backward) • TESTING POSITION: supine or prone • STIMULUS: When an infant looks down (neck flexion) or When an infant looks up (neck extension) • RESPONSE: causes the arms and legs to flex or curl into the body or this causes the arms and legs to extend (Superman) • ONSET :birth • INTEGRATED: 6months
Retained TLR • Challenges in creeping and crawling as an infant • Weakmuscles / low muscle tone • Decreased balance • Poor ocular motor skills • Visual-perceptual challenges • Decreased organization skills • Poor sense of space and time • Decreased sequencing • Frequent falls , bumping here and there • Spatial awareness difficulties • Dyscalculia and/or Dysgraphia
Integration • If your child is young, try engaging them in more tummy time activities: • Playing in front of the mirror. • Play ball in tummy time - roll the ball back and forth. • Try different animal crawls: worm crawl, snake crawl, etc. • Catch and thrown • Teach shapes and size
Challenges with organization, sense of time, and sequencing:Use more visuals. Visual schedules are great to help with sequencing and organizing tasks.Use pictures of where items belong to help with organization.Use visual timers to help with sense of time. • Ocular motor challenges: • Play more ball games. Instead of catch and throw, try bounce and catch or even rolling back and forth. • Reading with a highlighter strip or a piece of paper under the line that is being read. This helps the eyes focus on the line and decreases distracting visual input. • Decreased balance: • Practice! Complete activities on a balance beam or place a strip of painter’s tape on the floor and • Engage in core strengthening tasks using a therapy ball, jumping and climbing, and yoga stretches, etc.
Positive supporting reflex • TESTING POSITION: vertical position • STIMULUS: weight placed on ball of the feet when upright • RESPONSE: leg and trunk into extension • ONSET :birth • INTEGRATED: 6 months