Download
1 / 28
310 likes | 702 Views
Aligning Trial Design and Key Processes in Phase III Event Driven Trials: Protocol (via a Special Protocol Assessment), Data Monitoring Committee Charter & Statistical Analysis Plans. Barry Turnbull, PhD Principal Consultant. Abstract.

E N D
Aligning Trial Design and Key Processes in Phase III Event Driven Trials:Protocol (via a Special Protocol Assessment), Data Monitoring Committee Charter & Statistical Analysis Plans Barry Turnbull, PhD Principal Consultant
Abstract Coordination of an appropriate implementation of a clinical trial with regulatory authorities employing an event driven design can be a challenging effort. Often an IDMC is chartered for the trial monitoring and possibly the adaptation process creating another level of complexity. Often these event driven trials are pivotal in nature and trial sponsors are increasingly seeking the reduction in risk afforded by FDA's SPA process or protocol buy-in by CDRH or other regulatory bodies. Examples of alignment of key documents / processes plus negotiations with regulators of ”pivotal” event driven designs within the SPA process will be reviewed.
Definition of “Event” • Any objectively defined occurrence (one or more) of a measureable subject outcome • Known time of event not always known • Death vs. Disease Progression • Censoring Issues • Can have more than one event per subject • Hospitalization • Time to event (survival type analysis) most common analysis but not only event analysis • Negative binomial regression • Andersen - Gill
Powering Event Driven Trials • Based Purely on the Hazard Ratio • HR = (ln proportion alive at time t tx1) / (ln proportion alive at time t tx2)
Powering Event Driven Trials - continued • Based on Median Time to Event and Follow-up
Powering Event Driven Trials - continued • Can Include: • Accrual Time • Expected Dropout Rate / Censoring Pattern • User Specified Functions • Covariates / Proportional Hazards • Simulations • But Time to Event is NOT the Only Event Driven Endpoint
Adaptive Methodologies (increasing in frequency) Definition (PhRMA (2006), J. Biopharm. Stat., 16 (3), 275-283): “An adaptive design is referred to as a clinical trial design that uses accumulating data to decide on how to modify aspects of the study as it continues, without undermining the validity and integrity of the trial.” • Examples: • Sample Size Re-estimation • Interim Analysis (vs group sequential methodologies) • Overwhelming efficacy • Futility • Elimination of ineffective or “unsafe” doses / treatment arms • Adaptive Randomizations • Urn type / “play the winner” • Change analysis, endpoint, analysis population………
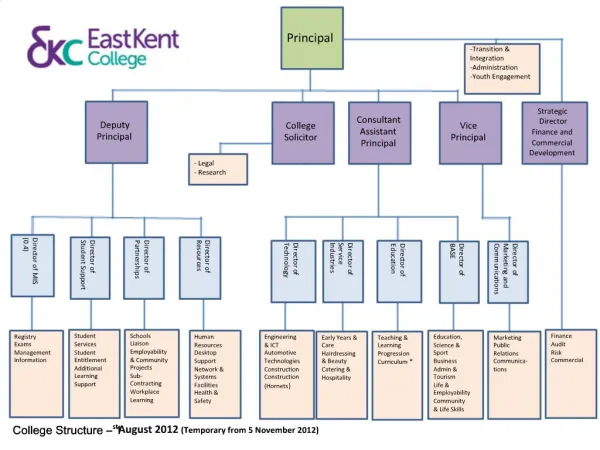
Groups Involved in the Event Driven Process* * Central Lab, CEC, Central Readers - possible
Special Protocol Assessment The PDUFA goals for special protocol assessment and agreement provide that, upon request, FDA will evaluate within 45 days certain protocols and issues relating to the protocols to assess whether they are adequate to meet scientific and regulatory requirements identified by the sponsor. “The clinical protocols for phase 3 trials can relate to efficacy claims that will be part of an original new drug application (NDA) or biologics license application (BLA) or that will be part of an efficacy supplement to an approved NDA or BLA.”
Key Trial Documents / Processes • Protocol / Study Design • Independent Data Monitoring Committee (IDMC) Charter • Statistical Analysis Plan (SAP) • IDMC SAP? • Case Report Forms / eCRFs? • Clinical Data Management Plan?
Negotiating with FDA via the SPA • Three Examples • Different FDA divisions within CBER and CDER • Different approaches by FDA staff • Different document requirements • Differing amounts of iterations among • Sponsor • FDA • CRO • IDMC (role can vary widely) • Different timelines
Example 1 • Company: Large Pharma Sponsor • Design: Randomized, Double Blind, PBO Controlled • Trial Size: Larger (n~600) • Primary Efficacy Endpoint: Disease Related Hospitalizations (multiple/pt) • Primary Efficacy Analysis: Negative Binomial Regression • Required number of events: 325 • IDMC Charter: Risk / Benefit (25%, 50%, 75%) • Stopping rule for futility (25% & 50%) • Stopping rule for overwhelming efficacy (25%, 50%, 75%) • Sample size re-estimation (50%)
Example 1 – continued • During the SPA review, FDA staff asked for: • Protocol only (included IDMC details) • Comments were received within ~30 Days • Interim analysis attempts too much • Stopping rule for efficacy not conservative enough and need to work with FDA if stopping rule met at interim • Need to account for safety hypotheses in stopping rule
Example 1 – continued • Protocol was updated and resent to FDA • FDA asked to meet regarding safety: • Desired staged enrollment and had detailed comments on the, not yet drafted, IDMC charter and IDMC statistical analysis plan (SAP) • FDA was sent updated protocol, plus newly drafted IDMC charter & IDMC SAP
Example 1 – continued • Study now has ~250 patients enrolled and we believe we have FDA agreement in all aspects of the design • Protocol design has been amended and FDA comments have not yet been received • CEC has been added to adjudicate efficacy and safety endpoints • SAP for trial when drafted will be sent to FDA and a meeting requested
Example 2 • Company: Smaller Biotech • Design: Randomized Double Blind, PBO controlled • Trial Size: Small (n~100) – Orphan Indication • Primary Efficacy Endpoint: Patent Reported Event • Primary Efficacy Analysis: Log-Rank Statistic • Required number of events: 60 • IDMC Charter: Risk / Benefit • Interim analysis (50%): • Stop for overwhelming efficacy • sample size re-estimation
Example 2 – continued • During the SPA, FDA (CDER) asked for: • Protocol • IDMC Charter • Approval was within ~50 Days • Pending acceptance of a few rounds of minor comments • Strongly suggested IDMC be blinded to the data
Example 2 – continued • Current Issues: • Sponsor accepted the IDMC being blind • Blinded assessment of variability of event distribution only results in limited information for sample size re-estimation • IDMC is very concerned about this methodology • stopping at interim for efficacy removed
Example 2 – continued • Current negotiating IDMC charter with IDMC members • They want direct access to FDA to convince them blinding them is not a good idea • Sponsor just wants to get going and is willing to solve these issues after study begins enrollment
Example 3 • Company: Larger Biotech • Design: Randomized, Open Label • Trial Size: Medium (n~400) • Primary Efficacy Endpoint: Survival • Primary Efficacy Analysis: Log Rank Statistic • Required number of events: 275 • IDMC Charter: Risk / Benefit • Interim analysis (25%, 50%, 75%) • Futility (25%) - conditional power • Overwhelming Efficacy (50%) • Sample size re-estimation (75%)
Example 3 – continued • During the SPA, FDA (CDER) asked for: • Protocol • IDMC Charter • SAP • CRFs
Example 3 - Continued • Approval was not received within 90 Days • FDA did not accept the interim analysis plan (on the second round of review; resetting the 45 clock) • FDA: “Irrespective of the scope of data dissemination, this is considered as three interim analyses, not one.” • The nominal p-value for the interim analysis at 50% of total required deaths was calculated by the statistical reviewer differently from that of the Sponsor
Example 3 - Continued • Revised protocol was submitted • IDMC would assess safety except for the 50% meeting • One efficacy interim at 50% • Removed futility analysis • Overwhelming efficacy – (using FDA’s calculated p-value) • Sample size re-estimation • Took 3 rounds and over 200 days to obtain agreement
Example 3 - Continued • Current Issues: • IDMC Concerns • Will not have access to efficacy analyses at 25% & 75% • Deaths (Safety & Efficacy) • Charter the IDMC worked on completely different from what was agreed to with FDA • No early futility analysis • Early sample size re-estimate
At the Interim Analysis – who can know what • It is a challenge to keep important information sequestered • Recall that the trial is based on the number of events not subjects / patients • Unblinded Staff: • IDMC • Unblinded Biostatistician (Sponsor or CRO, or both) • Perhaps a Stat programmer ((Sponsor or CRO, or both) • Work with Management Early • If the results require no change do X • If the result require increasing the trial size do Y • If the results require stopping the trial do Z • Etc. • Have Interim Analysis and IDMC SOPs in Place & Trained to
Summary • The SPA or other regulator negotiation processes, especially related to adaptive designs can be complex and time consuming. Sponsors should not expect agreement to be accomplished in a single meeting. • Combining IDMC function with adaptive designs creates the independence regulators desire but also creates several levels of logistical burdens. • One needs to carefully consider when to first involve the IDMC • FDA guidance encourages early involvement
Summary • There appears to be a need for increased constancy in terms of general protocol review process and the acceptance adaptive designs. • The SPA process in CDER and CBER does promote consistency and complete protocol review. The process CDRH and EU can be more time consuming and less definitive. • An ICH adaptive design guidance???