
Snakebite
E N D
Presentation Transcript
Snakebite Dr.Pratheeba Durairaj, M.D.,D.A,
Snake bite: an occupational disease • Farmers (rice) • Plantation workers (rubber, coffee) • Herdsmen • Hunters • Snake handlers (snake charmers and in snake restaurants and traditional Chinese pharmacies) • Fishermen and fish farmers • Sea snake catchers (for sea snake skins, leather)
How common are snake bites? • Many snake bites and even deaths from snakebite are not recorded. • One reason is that many snake bite victims are treated not in hospitals but by traditional healers. • India - No reliable national statistics are available. • In 1981, a thousand deaths were reported in Maharashtra State. In the Burdwan district of West Bengal 29,489 people were bitten in one year with 1,301 deaths. • It is estimated that between 35,000 and 50,000 people die of snake bite each year among India’s population of 980 million.
In the US: Snakebites frequently go unreported. The national average is approximately 4 bites per 100,000 persons. • Internationally: No accurate international data exist. Most snakebites and deaths due to snakebites are not reported.
Classification • Worldwide, only about 15% of the more than 3000 species of snakes are considered dangerous to humans. • The family Viperidae is the largest family of venomous snakes, and members of this family can be found in Africa, Europe, Asia, and the Americas. • The family Elapidae is the next largest family of venomous snakes.
Classification • There are two important groups (families) of venomous snakes in South East Asia • Elapidae have short permanently erect fangs This family includes the cobras, king cobra, kraits, coral snakes and the sea snakes. • The most important species, from a medical point of view include the following: • Cobras: genus Naja N naja(spectaled cobra –all over in India ) N kaouthia (monocled – West Bengal ,MP ,U.P, Orissa) N oxiana [Black cobra – northern states - patternless] N philippinensis N atra King cobra: Ophiophagus hannah
Spectacled Cobra Post synaptic Neurotoxin Good Response to Neostigmine
KRAITS (genus Bungarus) • B caeruleus common krait [all over India ] - paired white bands & large hexagonal scales in top of the snakes • B fasciatus banded krait [black & yellow band –W.B,M.P,A.P,BIHAR ,ORRISSA] • B candidus Malayan krait • B multicinctus Chinese krait • Sea snakes (important genera include Enhydrina, Lapemis and Hydrophis) • Blue spotted sea snake (Hydrophis cyanocinctus)
Common Krait Key identification feature are PAIRED white bands. Often enters human habitation Pre Synaptic Neurotoxin. Limited response to Neostigmine
Viperidae • Have long fangs which are normally folded up against the upper jaw but, when the snake strikes, are erected . • There are two subgroups, the typical vipers (Viperinae) and the pit vipers (Crotalinae). • The Crotalinae have a special sense organ, the pit organ, to detect their warm-blooded prey. This is situated between the nostril and the eye
Russell's Viper Haemotoxic venom BUT can also present neurotoxic symptoms Although nocturnal, encountered during the day, sleeping under bushes, trees and leaf particularly coconut leaf litter Key identification feature is the black edged almond or chain shaped marks on the back
Medically important species in South East Asia • Russell’s vipers -Daboia russelii - [Black edged chain like marking on body &white triangular marking on the head – throughout India] • Saw-scaled or carpet vipers - Echis carinatus and E sochureki [most parts of India except Kerala – Arrow shaped mark in head & hoop like markings in flanks ] • Pit vipers • calloselasma rhodostoma malayan pit viper • Hypnale hypnale hump-nosed viper • Green pit vipers or bamboo vipers (genus trimeresurus) • T albolabris white-lipped green pit viper • T gramineus indian bamboo viper • T mucrosquamatus chinese habu • T purpureomaculatus mangrove pit viper • T stejnegeri chinese bamboo viper
Key Identification Feature- large plate scales on the head. PIT VIPER Encountered under bushes and leaf litter or in bushes. Haemotoxic venom. Causes Renal failure Late onset envenoming No effective anti venom
How to identify venomous snakes • Some harmless snakes have evolved to look almost identical to venomous ones. • Some of the most notorious venomous snakes can be recognized by their size, shape, colour, pattern of markings, their behaviour and the sound they make when they feel threatened. • The defensive behaviour of the cobras is well known they rear up, spread a hood, hiss and make repeated strikes towards the aggressor.
CONTD… • Colouring can vary a lot. Some patterns, like the large white, dark rimmed spots of the Russell's viper ,or the alternating black and yellow bands of the banded krait are distinctive. • The blowing hiss of the Russell's viper and the grating rasp of the saw-scaled viper are warning and identifying sounds. • KRAIT bites : nocturnal, indoor, unprovoked & painless • COBRA & VIPER bites : painful & accompanied by neuroparalysis,coagulopathy
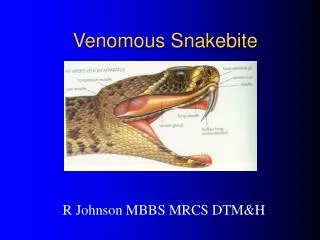
The venom apparatus • Venomous snakes of medical importance have a pair of enlarged teeth, the fangs, at the front of their upper jaw. • Venom is produced and stored in paired glands below the eye. It is discharged from hollow fangs located in the upper jaw. Fangs can grow to 20 mm in large rattlesnakes • These fangs contain a venom channel (like a hypodermic needle) or groove, along which venom can be introduced deep into the tissues of their natural prey. • If a human is bitten, venom is usually injected subcutaneously or intramuscularly. • Spitting cobras can squeeze the venom out of the tips of their fangs producing a fine spray directed towards the eyes of an aggressor.
Venom • Venom is mostly water. • Enzymatic proteins in venom impart its destructive properties. • Proteases, collagenase, and arginine ester hydrolase have been identified in pit viper venom. • Neurotoxins comprise the majority of coral snake venom. • Hyaluronidase allows rapid spread of venom through subcutaneous tissues by disrupting mucopolysaccharides; • Phospholipase A2 plays a major role in hemolysis secondary to the esterolytic effect on red cell membranes and promotes muscle necrosis
Contd… • Thrombogenic enzymes promote the formation of a weak fibrin clot, which, in turn, activates plasmin and results in a consumptive coagulopathy and its hemorrhagic consequences. • Enzyme concentrations vary among species, thereby causing dissimilar envenomations. • Copperhead bites generally are limited to local tissue destruction. • Rattlesnakes can leave impressive wounds and cause systemic toxicity. • Coral snakes may leave small wounds that later result in respiratory failure from the typical systemic neuromuscular blockade
CONTD… • ELAPID neurotoxins act at peripheral neuromuscular junction pre /post synaptically –prevent release of acetylcholine – prevents impulse transmission • VIPER –affect coagulation pathway at several points – Russels viper –activates V,IX,X,XIII factors ,platelets , protein C fibrinolysis
Quantity of venom injected at a bite • This Venom dosage per bite - is very variable - depends on the elapsed time since the last bite the degree of threat the snake feels the size of the prey. the species and size of the snake the mechanical efficiency of the bite whether one or two fangs penetrated the skin whether there were repeated strikes • The nostril pits respond to the heat emission of the prey, which may enable the snake to vary the amount of venom delivered.
Contd… • A proportion of bites by venomous snakes do not result in the injection of sufficient venom to cause clinical effects. • About 50% of bites by malayan pit vipers and russell’s vipers, 30% of bites by cobras and 5-10% of bites by saw-scaled vipers do not result in any symptoms or signs of envenoming. • Snakes do not exhaust their store of venom, even after several strikes, and they are no less venomous after eating their prey. • Although large snakes tend to inject more venom than smaller specimens of the same species, the venom of smaller, younger vipers may be richer in some dangerous components, such as those affecting haemostasis.
Pathophysiology • The local effects of venom serve as a reminder of the potential systemic disruption of organ system function. • Local bleeding - coagulopathies are not uncommon with severe envenomations. • Local edema - increases capillary leak and interstitial fluid in the lungs. Pulmonary mechanics may be altered • Local cell death - increases lactic acid concentration secondary to changes in volume status and requires increased minute ventilation. • The effects of neuromuscular blockade result in poor diaphragmatic excursion. • Cardiac failure can result from hypotension and acidosis. • Myonecrosis raises concerns about myoglobinuria and renal damage.
Symptoms and signs When venom has not been injected • Some people who are bitten by snakes or suspect or imagine that they have been bitten, may develop quite striking symptoms and signs, even when no venom has been injected. This results from an understandable fear of the consequences of a real venomous bite. • Anxious people may overbreathe so that they develop pins and needles of the extremities, stiffness tetany of their hands and feet and dizziness. • Others may develop vasovagal shock after the bite or suspected bite - faintness and collapse with profound slowing of the heart. • Others may become highly agitated and irrational and may develop a wide range of misleading symptoms.
Contd… • Another source of symptoms and signs not caused by snake venom is first aid and traditional treatments. • Constricting bands or tourniquets may cause pain, swelling and congestion. • Ingested herbal remedies may cause vomiting. • Instillation of irritant plant juices into the eyes may cause conjunctivitis. • Forcible insufflations of oils into the respiratory tract may lead to aspiration pneumonia, bronchospasm, ruptured ear drums and pneumothorax. • Incisions, cauterization, immersion in scalding liquid and heating over a fire can result in devastating injuries.
When venom has been injected! Early symptoms and signs • Following the immediate pain of mechanical penetration of the skin by the snake’s fangs, there may be increasing local pain (burning, bursting, throbbing) at the site of the bite • Local swelling that gradually extends proximally up the bitten limb • Tender, painful enlargement of the regional lymph nodes draining the site of the bite • Bites by kraits, sea snakes and Philippine cobras may be virtually painless and may cause negligible local swelling. • Symptoms and signs vary according to the species of snake responsible for the bite and the amount of venom injected
Local symptoms and signs • Fang marks • Local pain • Local bleeding • Bruising • Lymphangitis • Lymph node enlargement • Inflammation (swelling, redness, heat) • Blistering • Local infection, abscess formation • Necrosis
Generalised Symptoms and Signs • General • Nausea, vomiting, malaise, abdominal pain, weakness, drowsiness, prostration • Cardiovascular (Viperidae) • Visual disturbances, dizziness, faintness, collapse, shock, hypotension, cardiac arrhythmias, • pulmonary oedema, conjunctiva oedema
Snake bite: causes of hypotension and shock • Anaphylaxis - Vasodilatation • Cardiotoxicity • Hypovolaemia • Antivenom reaction • Respiratory failure • Acute pituitary adrenal insufficiency[In victims of Russell’s viper bites- haemorrhagic infarction of the anterior pituitary ] • Septicaemia
CONTD… Bleeding and clotting disorders (Viperidae) • Bleeding from recent wounds (including fang marks ,venepunctures etc) and old partly-healed wounds • Spontaneous systemic bleeding – from gums, epistaxis • Bleeding into the tears • Haemoptysis, haematemesis, rectal bleeding or melaena, Haematuria, vaginal bleeding • Bleeding into the skin and mucosae (petechiae,purpura,ecchymoses) • Intracranial haemorrhage
CONTD… • Renal (Viperidae, sea snakes) • Loin pain, haematuria, haemoglobinuria myoglobinuria, oliguria/anuria • Symptoms and signs of uraemia • Endocrine (acute pituitary/adrenal insufficiency) (Russell’s viper) • Acute phase: shock, hypoglycaemia • Chronic phase (months to years after the bite) loss of secondary sexual hair, amenorrhoea, testicular atrophy, hypothyroidism etc
Neurological (elapidae, russell’s viper) Drowsiness Paraesthesiae Abnormalities of taste and smell “Heavy” eyelids, ptosis External ophthalmoplegia Paralysis of facial muscles and other muscles innervated by the cranial nerves Aphonia Difficulty in swallowing secretions Respiratory and generalised flaccid paralysis Skeletal muscle breakdown (sea snakes, russell’s viper) Generalised pain Stiffness and Tenderness of Muscles, Trismus Myoglobinuria Hyperkalaemia Cardiac arrest Acute renal failure CONTD…
Complications • Compartment syndrome is the most frequent complication of pit viper snakebites. • Local wound complications may include infection and skin loss. • Cardiovascular complications, hematologic complications, and pulmonary collapse may occur. • Prolonged neuromuscular blockade may occur from coral snake envenomations.
Antivenin-associated complications • Immediate (anaphylaxis, type I) Result in laryngospasm, vasodilatation, and leaky capillaries - death • Delayed (serum sickness, type iii hypersensitivity reactions) • Serum sickness occurs 1-2 weeks after administering antivenin - arthralgias, urticaria, and glomerulonephritis • Usually more than 8 vials of antivenin must be given to produce this syndrome. • Supportive care consists of antihistamines and steroids.
Long term complications (sequelae) of snake bite • At the site of the bite, loss of tissue may result from sloughing or surgical debridement of necrotic areas or amputation • Chronic ulceration, infection, • Osteomyelitis or arthritis may persist causing severe physical disability • Malignant transformation may occur in skin ulcers after a number of years
Syndromic Approach • It is realised that the range of activities of a particular venom is very wide. For example, some elapid venoms, such as those of Asian cobras, can cause severe local envenoming , formerly thought to be an effect only of viper venoms. • In Sri Lanka and South India, Russell’s viper venom causes paralytic signs (ptosis etc) suggesting elapid neurotoxicity, and muscle pains and dark brown urine suggesting sea snake rhabdomyolysis. • There may be considerable overlap of clinical features caused by venoms of different species • “Syndromic approach” may still be useful, especially when the snake has not been identified and only monospecific antivenoms are available
SYNDROME 1 • Local envenoming (swelling etc) with bleeding/clotting disturbances = Viperidae (all species) • SYNDROME 2 • Local envenoming (swelling etc) with bleeding/clotting disturbances, • shock or renal failure = Russell’s viper and possibly saw-scaled viper - Echis species - in some areas) • with conjunctival oedema (chemosis) and acute pituitary insufficiency = Russell’s viper, Burma • with ptosis, external ophthalmoplegia, facial paralysis etc and dark & brown urine = Russell’s viper, Sri Lanka and South India • SYNDROME 3 • Local envenoming (swelling etc) with paralysis = cobra or king cobra
SYNDROME 4 • Paralysis with minimal or no local envenoming • Bite on land while sleeping, outside the Philippines = krait • in the Philippines = cobra(Naja philippinensis) • Bite in the sea = sea snake • SYNDROME 5 • Paralysis with dark brown urine and renal failure • Bite on land (with bleeding/clotting disturbance) = Russell’s viper, SriLanka/South India • Bite in the sea (no bleeding/clotting disturbances) = sea snake • Chronic renal failure occurs after bilateral cortical necrosis (Russell’s viper bites) and chronic panhypopituitarism or diabetes insipidus after Russell’s viper bites in Myanmar and South India
Management of snake bite • First aid treatment • Transport to hospital • Rapid clinical assessment and resuscitation • Detailed clinical assessment and species diagnosis • Investigations/laboratory tests • Antivenom treatment • Observation of the response to antivenom:decision about the need for further dose(s) of antivenom • Supportive/ancillary treatment • Treatment of the bitten part • Rehabilitation • Treatment of chronic complications
Aims of first aid • Attempt to retard systemic absorption of venom • Preserve life and prevent complications before the patient can receive medical care(at a dispensary or hospital) • Control distressing or dangerous early symptoms of envenoming • Arrange the transport of the patient to a place where they can receive medical care • ABOVE ALL, DO NO HARM!
FIRST AID –CONTD… • Unfortunately, most of the traditional, popular, available and affordable first aid methods have proved to be useless or even frankly dangerous. • Making local incisions or pricks/punctures (“tattooing”) at the site of the bite or in the bitten limb • Attempts to suck the venom out of the wound • Use of (black) snake stones • Tying tight bands [tourniquets) around the limb • Electric shock • Topical application of chemicals ,herbs or ice packs.
Tight (arterial) tourniquets are not recommended! • To be effective, these had to be applied around the upper part of the limb, so tightly that the peripheral pulse was occluded. • This method was extremely painful and very dangerous if the tourniquet was left on for too long (more than about 40 minutes), as the limb might be damaged by ischaemia- gangrenous limbs • Pressure immobilisation is recommended for bites by neurotoxic elapid snakes, including sea snakes but should not be used for viper bites because of the danger of increasing the local effects of the necrotic venom.
Tight (arterial) tourniquets are not recommended- WHY? • Confining this toxin in a smaller area, by use of compression techniques creates a greater risk of serious local damage. • When the tourniquet is removed there is the problem of the venom rapidly entering the system and causing respiratory failure in the case of neurotoxic bites • The Viper’s venom contains pro-coagulant enzymes which cause the blood to clot. In the small space below the tourniquet the venom has a greater chance of causing a clot. When the tourniquet is released the clot will rapidly enter the body and can cause embolism and death. • Lastly, there has been a great deal of research showing that tourniquets DO NOT stop venom from entering the body
Recommended first aid methods • Reassure the victim who may be very anxious • Immobilise the bitten limb with a splint or sling (any movement or muscular contraction increases absorption of venom into the bloodstream and lymphatics) • Consider pressure-immobilisation for some elapid bites • Avoid any interference with the bite wound as this may introduce infection,increase absorption of the venom and increase local bleeding
Pressure immobilisation method • An elasticated, stretchy, crepe Bandage,approximately 10 cm wide and at least 4.5 metres long should be used. • If that it not available, any long strips of material can be used. • The bandage is bound firmly around the entire bitten limb, starting distally around the fingers or toes and moving proximally, to include a rigid splint. • The bandage is bound as tightly as for a sprained ankle, but not so tightly that the peripheral pulse (radial, posterior tibial, dorsalis pedis) is occluded or that a finger cannot easily be slipped between its layers
Rapid clinical assessment and resuscitation • Airway, respiratory movements (Breathing) and arterial pulse (Circulation) must be checked immediately. • The level of consciousness must be assessed. • Urgent Resuscitation is needed in a) Profound hypotension and shock resulting from direct cardiovascular effects of the venom or secondary effects such as hypovolaemia or hemorrhagic shock. b) Terminal respiratory failure from progressive neurotoxic envenoming that has led to paralysis of the respiratory muscles. c) Sudden deterioration or rapid development of severe systemic envenoming following the release of a tight tourniquet or compression bandage d) Cardiac arrest precipitated by hyperkalaemia resulting from skeletal muscle breakdown (rhabdomyolysis) after sea snake bite.