Download
1 / 65
840 likes | 1.3k Views
Gastric Cancer. 浙江大学附属第一医院 胃肠外科 于吉人. Ji-Ren Yu Department of GI Surgery, The First Affiliated Hospital, Zhejiang University. Epidemiology. The fourth most common cancer worldwide The second most common cause of death from cancer.

E N D
Gastric Cancer 浙江大学附属第一医院 胃肠外科 于吉人 Ji-Ren Yu Department of GI Surgery, The First Affiliated Hospital, Zhejiang University
Epidemiology • The fourthmost common cancer worldwide • The second most common cause of death from cancer • Higher rates in Eastern Asia, South America, Eastern Europe • Lower rates in Western Europe and the United States
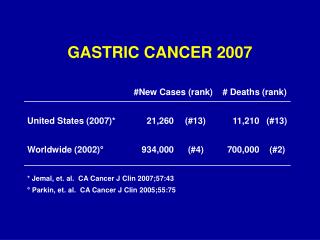
Epidemiology Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011; 61:69.
Nutritional Low fat or protein consumption Salted meat or fish High nitrate consumption High complex carbohydrate consumption Causes
Environmental Poor food preparation (smoked, salted) Lack of refrigeration Poor drinking water Smoking Causes
Medical Prior gastric surgery H. pylori infection Gastric atrophy and gastritis Adenomatous polyps Other Male gender Low social class Causes
i) Early gastric cancer(EGC) Pathology Gastric cancer confined to the mucosa or submucosa, regardless of the presence or absence of lymph node metastasis ii) Advanced gastric cancer(AGC) Cancer cells infiltrate the proprial muscle layer or serosa
EGC Pathology I: protruded IIc: superficially depressed III: excavated IIa: superficially elevated IIb: superficially flat
EGC:Endoscopic images Type I Type II Type III
Pathology AGC:Borrmann’s classification Linitis plastica
Photomicrographs of Gastric Carcinoma H&E, ×25 H&E, ×400 Arrows on signet ring cells
Metastesis Direct invasion Lyphmatic metastesis Hematogenous metastasis Seeding metastasis
Clinical Presentation Lacks specific symptoms early: vague epigastric discomfort indigestion. Epigastric pain, nonradiating, and unrelieved by food ingestion. Weight loss, anorexia, fatigue, or vomiting. Hematemesis, anemic. Large bowel obstruction.
Physical signs i) A palpable abdominal mass ii) A palpable supraclavicular or periumbilical lymph node ii) Peritoneal metastasis palpable by rectal examination iii) A palpable ovarian mass (Krukenberg's tumor). iv) Jaundice, ascites, and cachexia.
Endoscopy M-SCT (multiple spiral CT) BUS & EUS Double-contrast radiography MRI DL (diagnostic laparoscopy ) PET-CT Investigations
Endoscopy Carcinoma in situ Advanced carcinoma
Niche Double-Contrast Barium Upper GI Radiography
EUS T N T
A B C N M T CT scan T4N2M1
Laparoscopy T T Abdominal metastasis
BUS left right right Liver metastasis Krukenberg’s tumor
PET/CT T3N2M0
Treatment for Gastric Cancer Surgery Endoscopic mucosal resection (EMR) Endoscopic submucosal dissection (ESD) Laparoscopic Surgery Open Surgery Chemotherapy Chemoradiotherapy Target therapy
Principles of radical operation for gastric cancer i) Negative margin ii) Extent of lymph node dissection iii) Enbloc resection Surgical Treatment for Gastric Cancer
Criteria for EMR • NCCN 2014 V1: • 1.Tis or T1a • 2. Well or moderately differentiated histology • 3.Tumors less than 20mm in size • 4. Clear margins • 5.No evidence of invasive finding
Criteria for EMR Japanese Gastric Cancer Association • Absolute indication (EMR/ESD): • Differentiated adenocarcinoma • T1a • diameter is ≤2 cm • without ulcer finding (UL-) • Expanded indication (ESD): • Tumors clinically diagnosed as T1a and: • (a) Differentiated, UL( - ), but>2 cm • (b) Differentiated-type, UL(+), and ≤ 3 cm • (c) Undifferentiated-type, UL(-), and ≤ 2cm
1. Difficult to resect large than 20mm tumor in size 2. Difficult to resect ulcerative lesions Limitation of EMR techniques ESD has been developed
Laparoscopic Resection 1) A suitable procedure for ECG; 2) The efficacy and safety of this approach for advanc gastric carcinoma requires further investigation
Open Surgery for Advanced Gastric Cancer 1. A suitable procedure for ACG 2. R0 resection 3. R1 resection 4. R2 resection
Principles of radical operation Gastrectomy with regional lymphatics: perigastric lymph nodes(D1) and those along the named vessels of the celiac axis (D2), with a goal of examining 15 or greater lymph nodes Gastrectomy with D2 lymphadenectomy is the standard treatmentfor curable gastric cancer in eastern Asia
Gastrectomy and D2 lymphadenectomy for advanced gastric carcinoma Gastrectomy
Anastomosis Billroth II anastomosis Roux-en-Y anastomosis Subtotal gastrectomy
Left gastric A Hepatic A Splenic A No.11 LN