Download
1 / 26
310 likes | 579 Views
Mathematical Modelling of Radiotherapy: Applying the LQ model. Helen McAneney 1,2 & SFC O’Rourke 2. 1 School of Medicine, Dentistry and Biomedical Sciences 2 School of Mathematics and Physics. Background. Radiation treatment is second after surgery in battle against cancer growths

E N D
Mathematical Modelling of Radiotherapy: Applying the LQ model. Helen McAneney1,2 & SFC O’Rourke2 1School of Medicine, Dentistry and Biomedical Sciences 2School of Mathematics and Physics
Background • Radiation treatment is second after surgery in battle against cancer growths • Success at killing cells, both cancerous and normal cells • Fractionated treatment schedules • Treatment planning involves • Localizing, Imaging, Identifying, Optimizing, calculations and reporting www.n-i.nhs.uk/medicalphysics
Constant Repopulation? • Typically, the tumour sensitivity and repopulation are considered to be constant during radiotherapy. • Exponential re-growth has constant growth kinetics. • Suggested that cell cycle regulation and anti-growth signals (hypoxia) reduce response to radiotherapy • S-phase of cell cycle, • low levels of oxygenation • Nutrient deprived cells are less apt at mitosis, therefore, as the tumour shrinks and re-oxygenation occurs to areas previously deprived, the net repopulation rate will increase • Implies repopulation rate that is not constant throughout the course of therapy
Non-constant repopulation • One example of this may be found in some human lung cancers which have been shown by Steel (1977, 2002) to follow a Gompertzian pattern of growth. • It has been shown that larger tumours have longer volume doubling times than smaller ones (Steel 1977, Spratt et al 1993).
Growth Laws • Various Growth Laws for tumour growth include • Exponential • Logistic (*) • Gompertz (*) • Does the nature of the re-growth of tumour between treatments effect outcome? • Is prognosis similar or different than when exponential re-growth is considered?
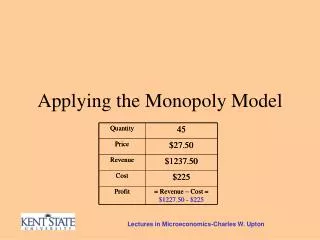
LQ Model • Linear-Quadratic model • a and b characterise tissue’s response to radiotherapy. D is dose in Gy Typical a/b = 3 -10 Gy Adv. Head & neck a/b = 20 Gy Non-small-cell lung a/b = 10 Gy Prostate a/b = 1 Gy
5 R’s of radiotherapy Repair, repopulation, re-distribution, re-oxygenation, intrinsic radio-resistance AQ4N unique bioreductively activated prodrug converted to a persistent anticancer agent unaffected by tumour re-oxygenation “most promising anticancer bioreductive drug in preclinical development” 5 R’s and AQ4N British Journal of Cancer (2000) 83, 1589–1593. doi:10.1054/bjoc.2000.1564 (Review) Clinical Cancer Research 14, 1096-1104, 2008. doi: 10.1158/1078-0432.CCR-07-4020 (Phase I trial)
Re-distribution and Re-oxygenation • Re-distribution • Asynchronous cycling cell population, preferentially spare cells in resistant part of cell cycle • ‘Split-dose’ expt., time between fractions increased by • A few hours: SF increases as sublethal damage repaired • Cell cycle time: SF decreases as cells re-distribute, killed on 2nd exposure. • Re-oxygenation • Surviving hypoxic cells move to more sensitive (oxic) state before next exposure
Re-sensitization • ‘Post irradiation increase the sensitivity of cells that survive an initial partial exposure’ • Occurs when • An early part of a radiation exposure leads to a decreased average radiosensitivity just after the dose is administered, ie kills the more radiosensitive cells of a diverse population. • Subsequent biologically driven changes gradually restore the original population average radiosensitivity. Hlatky 1994, Brenner et al 1995
LQR model • Before irradiation, a has Gaussian probability distribution, variance s2 • After irradiation, a still Gaussian, variance s2, but average value decreased, as resistant cells are preferentially spared • Averaging over subpopulations gives • Increase in SF due to cell to cell diversity. • Extra resistance of particular resistant cells ‘outweighs’ extra resistance of particularly sensitive cells. Hlatky 1994, Brenner et al 1995
2-compartment LQR model • Heterogeneity of cells: Hypoxic cells, re-oxygenation etc. • Two-compartment LQR model, assuming bi-variate Gaussian distribution oxic Ro hypoxic Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
2-compartment LQR model • Heterogeneity of cells: Hypoxic cells, re-oxygenation etc. • Two-compartment LQR model, assuming bi-variate Gaussian distribution • Proliferation of oxic cells, but not hypoxic, oxic hypoxic Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
2-compartment LQR model • Heterogeneity of cells: Hypoxic cells, re-oxygenation etc. • Two-compartment LQR model, assuming bi-variate Gaussian distribution • Proliferation of oxic cells, but not hypoxic, yet region increases due to viable rim of nutrients oxic Ro hypoxic Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
2-compartment LQR model • Heterogeneity of cells: Hypoxic cells, re-oxygenation etc. • Two-compartment LQR model, assuming bi-variate Gaussian distribution • Treatment: radio-resistance of hypoxic cells, oxic hypoxic Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
2-compartment LQR model • Heterogeneity of cells: Hypoxic cells, re-oxygenation etc. • Two-compartment LQR model, assuming bi-variate Gaussian distribution • Treatment: radio-resistance of hypoxic cells, yet redistribution and re-oxygenation occurs. oxic Ro hypoxic Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
Local sensitivity • Table 1, proposed expressions for the local sensitivity for the three studied models, whose denomination comes from their dependence with position r. • α0 and β0 are parameters of each model related with the oxygenation level at the tumour surface. Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
Overall radiosensitivity • Ensemble average and volumetric average are interchangeable, supposing that operating over sufficiently large volumes. Then Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
Overall radiosensitivity: two zones Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
Viable rim r0 of 50 mm for all tumour sizes. ‘Constant crust’ model. • and ( and ) estimated by least squares fit to experimental data (Buffa et al) for spheroid with R = r0 = 50 μm in oxic (hypoxic) conditions • Oxic fraction given by Horas et al Phys. Med. Biol. 50 (2005) 1689-1701
Fortran 90 language Lagrange Interpolation : Aiken algorithm Relating R to N volume of tumour volume of cell Weighted averages of oxic and hypoxic parameters to obtain homogeneous parameters Repopulation: Exponential, Logistic, Gompertz Treatment schemes: Uniform, standardised, accelerated etc. Programming
A few results Accelerated treatment - LQR Linear local sensitivity
A few results Accelerated treatment - LQ Linear local sensitivity
A few results Accelerated treatment - % dif Linear local sensitivity
A few results Quadratic Model of local sensitivity LQR LQ Parameter values: R0=375 mm, D=2 Gy, t2=80 days, weekday treatments for 6 weeks. (left) Changing dynamics, proportions and therefore radio-sensitivity parameters of subpopulations within tumour throughout treatment schedule given different types of repopulation. (right) Fixed radio-sensitivity parameters at start of treatment schedule determined by weighted averages for different types of re-growth laws.
Questions • Though cells more radio-resistant via hypoxia, less growth occurs also. Balances..? Dominate feature? Will hypoxia increase or decrease the effectiveness of radiotherapy? • How effective is accelerated fractionation compared to standard fractionation on heterogeneous tumours? • Does the level of heterogeneity of the tumour matter?
Joe O’Sullivan Francesca O’Rourke Anita Sahoo Frank Kee - Director Centre of Excellence for Public Health NI Leverhulme Trust Acknowledgements • Publications • H. McAneney and S.F.C. O’Rourke, • Investigation of various growth mechanisms of solid tumour growth within the linear-quadratic model for radiotherapy, Phys. Med. Biol. 52, (2007), 1039-1054. • S.F.C. O’Rourke, H.McAneney and T. Hillen, • Linear Quadratic and Tumour Control Probability Modelling in External Beam Radiotherapy, J. Math. Biol. doi 10.1007/s00285-008-0222-y • S.F.C. O’Rourke, H.McAneney, C.Starrett and J.M. O’Sullivan, • Repopulation Kinetics and the linear-quadratic Model, • American Institute of Physics Conference Proceedings, accepted Aug 2008.