Download
1 / 38
430 likes | 654 Views
Health care financing for the poor in Lao PDR. Student: Walaiporn Patcharanarumol Supervisor: Prof. Anne Mills. Outline of presentation. Introduction User fees and protection mechanisms Lao People’s Democratic Republic Objectives Conceptual framework and Methodology Work plan and budget.

E N D
Health care financing for the poor in Lao PDR Student: Walaiporn Patcharanarumol Supervisor: Prof. Anne Mills
Outline of presentation • Introduction • User fees and protection mechanisms • Lao People’s Democratic Republic • Objectives • Conceptual framework and Methodology • Work plan and budget
Introduction • The poor and the health: policy agenda cause Ill health Poverty effect
Introduction • The mitigation of impact of user fees on access to health services by the poor • Main focus of the study: protecting the poor from the financial burden of user fees charged for public health care services.
What is user fee? • User fees are payments made by individuals or families at point of service for buying health care services with whatever form of charge and at whatever level of public health care provision
User fees • The policy aim: revenue raising, improving health system efficiency and enhancing equity in access to the health system • The main source of health services financing in some countries • Can be a financial barrier which leads to inequity in access to health care services
Experiences on user fees and exemptions • User fees improved hospital services • However, user fees represented barrier in access to health services, especially for the low socio-economic group. It created a medical poverty trap • Ineffective exemption mechanisms • Inadequate funding • A limitation of administrative capacity • Insufficient information • Stigmatization • Staff awareness • Optional mechanisms e.g., the Health Equity Fund, Universal Health Care Coverage
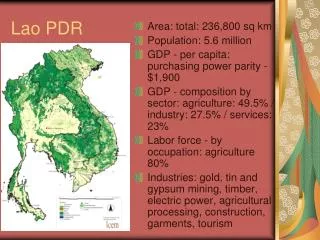
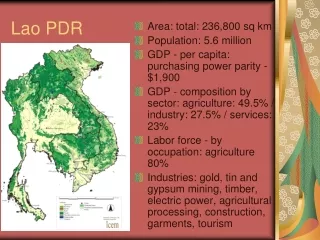
Lao PDR • Lao PDR: one of the Least Developed Countries (LDCs) • 5.3 million population • Life expectancy at birth: 54.3 years • Adult literacy rate: 66.4% • Poverty: 32.7% of total pop (National poverty line = 8.5 USD/person/mo)
Health care delivery system in Lao PDR 1. Public health facilities • 533 Health centers • 122 District hospitals • 13 Provincial hospitals • 5 regional and 6 specialized hospitals • 3 Central hospitals A district hospital in Savannakhet Province 2. Private sector • 1990 licensed pharmacies and 261 private clinics • No private hospital
Health care financing in Lao PDR • Total health expenditure: 3% of GDP, 12 USD per capita • Household OOP: 58% of total health expenditure • 1/3 of OOP was spent on user fees in public providers • No national health insurance scheme • Government employee scheme: 16% of total pop • Social health insurance: <1% of total pop • Community based health insurance: 0.2% of total pop (pilot) • Most people has no health insurance and they are directly faced with user fees at point of service.
User fees and exemptions in Lao PDR • Decree 52 on Medical Services and Guide of the Public Health Minister, 1995 • Cost recovery in hospital was introduced to generate revenue • School children and students, monks and poor people are exempted from paying • Hospitals are allowed to keep up to 80% of their revenues from user charges (20% of revenue from user charges goes to local government)
User fees and exemptions in Lao PDR • User charges: • Drugs at cost plus 25% margin • Other services such as laboratory, radiology, admission and surgery with a fixed fee schedule. • Exemption mechanism is not functioning: the poor lack knowledge and believe that exemption is unrealistic • Vientiane Time: “people do not come to the hospital when they have no money unless they have a serious health problem”
What do we know? What’s next?
Gap of knowledge • No clear evidence whether exemption influences the poor’s coping strategies or not. Most studies haven’t looked atdemand side • Why households do / do not take up exemptions. • Which factors might encourage the poor to take up exemptions? • There has been little exploration of provider motivations to grant exemptions. • Little research has been conducted with a comprehensive view from households, health care providers and policy makers • No comprehensive analysis inLao PDR
Objectives • To assess the perceptions and preferences of national policy makers on fee exemption policy and implementation. • To assess public health care providers’ behaviour and attitudes on exemption mechanisms • To analyze barriers of access to public health care services, utilization patterns and household illness costs by socio-economic group.
Objectives (continued) • To assess the strategies households use to cope with medical bills with an emphasis on taking up the exemption mechanism. • To analyse the financial implications of alternative protection mechanisms. • To identify policy implications for pro-poor financing and provide policy recommendations on improved ways of protecting the poor.
Government (Policy maker perspective) Health system (Supply-side perspective) Household/community (Demand-side perspective) Conceptual Framework Policy recommendation Public health care expenditure implication Policy options for protecting the poor Public Health care financing Utilization pattern Government (Policy maker perspective) Health system (Supply-side perspective) Household/community (Demand-side perspective) Treatment seeking pattern Illness Policies on health care financing and exemption policy • Public health care providers • - Health Centre - District Hospital • Provincial • Hospital Barriers on access to health care services Cost of Illness Impact on household budget Coping strategies for treatment cost of illness Take up? Supply-side design and implementation Policy design and implementation Exemption mechanism Demand-side design and implementation 6
Study setting • National Growth and Poverty Eradication Strategy (NGPES), Lao PDR 2004 • Totally 142 districts are classified into three groups • Very poor • Poor • Non poor Savannakhet Province
Study setting • Savannakhet Province • Very poor or poor districts • Why Savannakhet Province? • Safety • Possible to travel • No dialect problem Savannakhet Province
Methodology Supply-side perspective 1. National policy makers (qualitative method) 2. Providers (quantitative and qualitative methods) Demand-side perspective 3. Households (quantitative and qualitative methods) Synthesis 4. Financial modeling
The first sub-study: national policy makers Objectives • Existing exemption policy (funding, design, implementation) • Attitudes on user charges and exemption policy • Policy options for protecting the poor Tool • Key informant interviews using semi-structured Q’naire
The first sub-study: national policy makers Variables (examples) • The purpose of user fees • Who controls the fee policy? • Existence and clarity of national policy on exemption, resource, benefit package • Who decides means testing? What criteria are used for means testing? • Relationship between criteria and national poverty criteria • Responsiveness of eligibility criteria to local circumstances • Effective exemption mechanism, how to finance (tax, pre-payment), which option is feasible, not feasible, who and what package will be protected, priority setting
The second sub-study: public health care providers • Both quantitative and qualitative methods will be applied to obtain all important information from all levels of public health care providers. • Quantitative data: financial data, revenue from user fee, exemption (+/- debt) • Qualitative data: attitude and practice on user fee and exemption, factor affecting exemption in practice
The third sub-study: household side • Three methods are applied to obtain information from household side • Analysis of national survey • Rapid rural appraisal • Household case studies
The third sub-study: household side Analysis of national survey Objectives • To quantify household members’ information on morbidity rate, use of health services, cost of treatment and transportation cost by socio-economic group • To determine cost of treatment as % of household income or expenditure
The third sub-study: household side Rapid rural appraisal (RRA) • It is aimed at exploratory research • to generate baseline data • to handle complicated information sets • to rank lists of items such as foods and • to understand variation and complexity within field settings (Seaman, Clarke et al. 2000)
The third sub-study: household side Rapid rural appraisal (RRA) • It emphasizes the use of • existing data • interaction with local residents and • a judicious combination of qualitative methods. • Tools • semi-structured key informant interviews • focus group discussions • supplemented by observation, photographs, and a preliminary review of secondary data. • Various techniques e.g., social mapping, wealth ranking with card sorting, and preference ranking
The third sub-study: household side Household case studies (by in-depth interview) Objectives • To measure costs of treatment in the hospital paid by the household • To explore coping strategies used by the household to deal with financial costs of illness • To explore experience and probe attitudes of households on exemptions • To investigate other barriers of access to health care services
The third sub-study: household side Household case studies (by in-depth interview) DH = district hospital, PH = provincial hospital * for example death (from disease) at home, giving birth at home without birth attendance
The fourth sub-study: financial modelling Objective • To analyze financial implications for health care providers’ budgets of various options for protection mechanisms Data/information needed • Coverage data: size and structure of entitled population by protection mechanism • Utilization data: pattern and intensity of the utilization • Benefit package and amount of benefit data: over a certain period of time. • Expenditure and revenue data
The fourth sub-study: financial modelling Possible dummy table
Exemption level Less leakage Diagram of samples and methods KI interview National level MOH and NIPH One provincial hospital KI interview, FDG and financial data collection Provincial level Financial data collection District level in the province All district hospitals 4 district hospitals (low and high exemptions) KI interview, FDG and financial data collection 1 district hospital with low exemptions 1 district hospital with high exemption 12 households for case study 12 households for case study In-depth interview In-depth interview Village level in the 2 districts Some health centers Some health centers KI interview, FDG and financial data collection
Collaboration • National Institute of Public Health, Lao PDR • Provincial Health Department: Savannakhet Province • Savannakhet Provincial Hospital • District Health Office (two districts)
Work plan and budget • Duration of fieldwork: 10 months from Oct 05 - July 06 • Total budget requirement for the fieldwork ~ 900,000 baht • All costs are covered by Dorothy Hodgkin Postgraduate Award 2004.
Acknowledgement • To Prof. Anne Mills for her intellectual guidance and continuing supervision. • To advisory committees, Dr. Steve Russell and Dr. Catherine Goodman, for their supports and suggestions • To DHPA for financial support of my PhD studies • To IHPP-Thailand