Download
1 / 35
390 likes | 491 Views
Learn about the causes, symptoms, and prevention of meningococcal infection, an acute disease that predominantly affects children under 5 years old. Discover the epidemiology, classification, and diagnosis of this serious illness.

E N D
Meningococcal infection Part 1 • Lecturer Bynda Tatyana
Professional motivation • Meningococcal infection - is a hard disease, mostly occurs in children under 5 years old (70% of cases), because of bad immune reactivity. • During last decades meningococcemia or combined forms has increased, they lead to unfavourable results more often.
Professional motivation • Prognoses of the disease, mortality depend on in time diagnostic, hospitalization and treatment. • It requires from the doctor to know diagnostic criterion’s duration, treatment and prevention of this pathology.
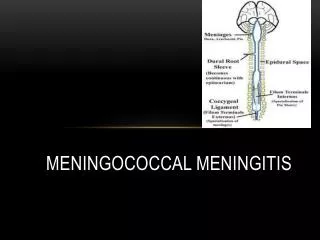
Meningococcal infection • Meningococcal infection is an acute infectious disease characterized by a variety of clinical forms, from nasopharyngitis to extensive forms such as meningococcemia, meningitis, meningoencephalitis, and more rarely with involvement of other organs and systems.
Etiology: • The causative agent of the infection is a Gram-negative diplococcus from a species Neisseria meningitides (Weichselbaum’s meningococcus), which is divided into 13 groups (A, B, C, D, Z, X, and Y) according to antigenic structure.
Etiology: • Most often the disease is caused by a meningococcus of group A, in recent years of groups B and C. • Epidemic outbreaks of the disease are associated with the type A.
Etiology: • Meningococcus is very unstable in external environment and outside the human body dies in 30 minutes. • Toxic properties of meningococcus are due to endotoxin • Meningococcus grows on nutrient medium containing human protein (blood serum or ascitic fluid) .
Epidemiology • The sources of infection are patient and carriers who expel the causative agent with the secretions from the nasopharynx and upper respiratory passages (sneezing, coughing, speaking).
Epidemiology • Infection is usually conveyed by the aerial-droplet route, direct contact. • The susceptibility of man to meningococcal infection is slight. • The susceptibility index does not exceed 10-15 %. • Only 15% of contact persons may be infected, 98% of them become carriers, only 2% - ill.
Susceptibility • Susceptibility is high in children 6 months - 5 years old. • The highest incidence - in Africa, especially in Central and Western (so-called "meningitis belt").
Susceptibility • Meningococcal disease occurs in 155 countries around the worldEvery 10 - 30 years there has been increasing of morbidityMorbidity: • in Europe - 5 to 100 000 population • Africa - 20 to 100 000 population • in Ukraine - 8-10 to 100 000 population
Epidemiology Seasonal elevations are noted in winter and spring. Nowadays meningococcal infection occurs sporadically Postinfectious immunity is stable The meningococcal infection is characterized by periodic rises of the incidence 10–15 years or longer.
Pathogenesis 1. Inoculations and reproduction of bacteria in upper respiratory tract. The portal of entry is the nasopharyngeal mucosa. 2. Local inflammation, lymphoid tissue hyperplasia (nasopharyngitis). 3. Bacteraemia, dissemination. 4. Toxemia (meningococcemia). 5. Rupture of hematoencephalic barrier (meningitis, meningoencephalitis).
Meningococcal Infections The incubation period lasts for 3–5 days on average (maximum 10 days).
Classification of Meningococcal Infection: • Localized forms • Meningococcal carrying, • Acute nasopharyngitis; • Generalized forms
Classification of Meningococcal Infection: • Generalized forms Typical • meningococcemia, • meningitis, • meningoencephalitis. • Combined (or mixed) forms (meningitis + meningococcemia or meningoencephalitis + meningococcemia). Atypical • fulminant form • chronic meningococcemia
Classification of Meningococcal Infections: • Rare forms endocarditis, arthritis, pneumonia, iridocyclitis.
How to word a diagnosis (an example): • Meningococcal infection, localized form, acute nasopharyngitis. • Meningococcal infection, generalized, typical, combined form: meningitis, meningococcemia.
Nasopharyngitis • The most frequent form of the manifest meningococcal infection is nasopharyngitis. Nasopharyngitis is characterized by • an acute onset, • absence of general toxicosis, subfebrile body temperature, • headache, • catarrhal syndrome.
Nasopharyngitis: catarrhal syndrome • painful swallowing, • hyperemia of the nasopharyngeal mucosa and hyperplasia of lymphoid nodes, • rhinitis with scanty discharge, and • difficult nasal breathing. The course is favorable, and the patient recovers in 5-7 days, but in 30-40% of cases it may transform into an extensive form.
Meningococcemia • is characterized by the most acute onset. The parents always know the exact time when the child fell ill. • Toxicosis is extremely marked since the first hours. • The temperature elevates up to 39-40°C; there is sudden fatigue, motionlessness, headaches, and hyperesthesia of the skin.
Meningococcemia • Sometimes before hemorrhagic eruption, there are roseolas and papules, which disappear during the 2nd day. • It complicates making diagnosis and may lead to a false diagnosis.
Meningococcemia Eruption develops 6-12 hours, sometimes about 24 hours after the beginning of the disease. Most often, the first eruption is localized on the buttocks, posterior surface of the thighs and shins, and then spread to the whole body very quickly.
Lesions are more common on the trunk and extremities but may also occurs on the palms, soles and mucosa.
Meningococcemia The eruption is hemorrhagic, from petechiae to large hemorrhages, star-shaped, with necrosis in the center, and uneven ragged edges.
Meningococcemia In extensive and deep necrosis there is rejection of necrotic parts of the tissues; there may be necrosis of finger-tips, hands, auricles, and feet.
Meningococcemia • There may be hemorrhages into the joints, sclerae, and parenchymatous organs.
Waterhouse-Friderichsen syndrome • In Waterhouse-Friderichsen syndrome, the clinical signs of septic shock develop during several hours; there is much hemorrhagic eruption on the face. The eruption develops very quickly. • Consciousness is impaired rapidly, from somnolence to sopor. • Tachycardia, arterial hypotonia, decreased diuresis are quite marked.