Download
1 / 54
540 likes | 744 Views
CLINICAL PHARMACY IN RHEUMATOLOGY. RHEUMATIC DISEASES. Rheumatic diseases (rheumatism) are painful conditions that affect millions. These diseases cause inflammation, swelling, and pain in the joints or muscles.

E N D
RHEUMATIC DISEASES • Rheumatic diseases (rheumatism) are painful conditions that affect millions. These diseases cause inflammation, swelling, and pain in the joints or muscles. • Some rheumatic diseases like osteoarthritis are the result of "wear and tear" to the joints. Other rheumatic diseases, such as rheumatoid arthritis, happen when the immune system goes haywire; the immune system attacks the linings of joints, causing joint pain, swelling, and destruction.
Rheumatism is a medical term once frequently used to describe disorders associated with many different parts of the body. Most often, people associate rheumatism with arthritis, or with rheumatic fever, a complication of strep throat that can result in damage to the heart. However, the term rheumatism might apply to the symptoms of numerous conditions that can cause pain and/or weakness. • Some conditions that were once given the general label of rheumatism or called rheumatic diseases include, rheumatoid arthritis, osteoarthritis, lupus, fibromyalgia, and tendonitis. Frequently autoimmune disorders, since they remained unnamed but caused pain as well as affecting other organs, were classed as rheumatism. Illnesses like lupus were particularly susceptible to being called rheumatism. Later understanding of the actions of these illnesses show that the problem is not dysfunction of the joints, but rather immune systems that can attack joints, muscles and organs.
Some forms of rheumatism are called non-articular rheumatism and may affect the soft tissues causing pain throughout the body. Conditions like tendonitis and fibromyalgia fall into this category. As well, non-articular rheumatism can be localized to specific areas in the body. Bursitis is a non-articular form of rheumatism that affects and inflames the bursa, which are special sacs that protect joints and overlapping muscles. Bursitis most frequently occurs at the site of one joint that may have been injured through overuse.
Osteoarthritis OA is not a normal part of aging; it usually affects the knees, hips, lower back, neck, and fingers. • The signs and symptoms of OA include: • Pain in joint • Joint swelling • Joint may be warm to touch • Joint stiffness • Muscle weakness and joint instability • Pain when walking • Difficulty gripping objects • Difficulty dressing or combing hair • Difficulty sitting or bending over To diagnose OA, doctor will ask the patient about medical history and symptoms and do a physical exam. Blood tests may help rule out other types of arthritis or medical problems. A joint fluid sample from an affected joint may also be examined to eliminate other medical problems.
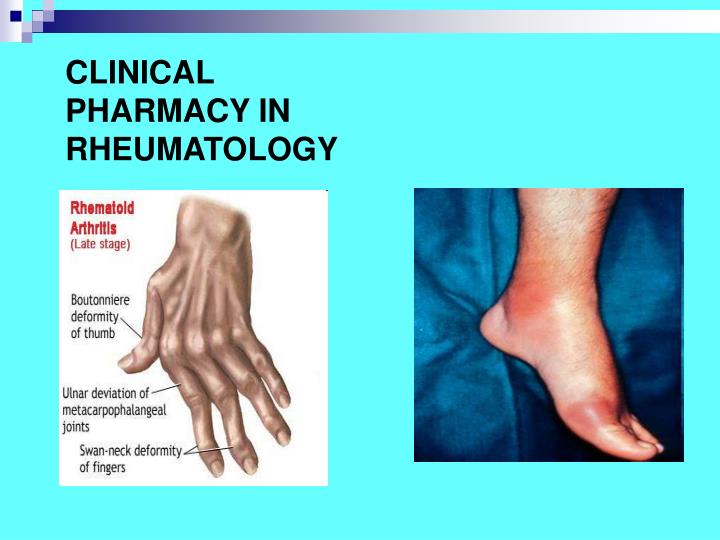
Rheumatoid Arthritis RA is sometimes called a crippling disease. That's because it can result in permanent joint damage and deformity. RA signs and symptoms include: • Joint pain, stiffness, and swelling • Involvement of multiple joints (symmetrical pattern) • Other organ involvement • Joint stiffness, especially in the morning • Fatigue • Fevers • Lumps called rheumatoid nodules To diagnose RA, doctor will ask about medical history and do a physical examination. Also, X-rays and blood tests will likely be taken. One blood test may be for rheumatoid factor; it is positive in 70% to 80% of those with RA.
Lupus SLE or systemic lupus erythematosus is another autoimmune disease; the cause of SLE is unknown. Lupus signs and symptoms include: • Joint pain • Fatigue • Joint stiffness • Rashes, including the"butterfly rash" across the cheeks • Sun sensitivity • Hair loss • Discoloration of the fingers or toes when exposed to cold (called Raynaud's phenomenon) • Internal organ involvement, such as the kidneys • Blood disorders, such as anemia and blood clots • Chest pain from inflammation of the lining of the heart or lungs • Seizures or strokes To diagnose lupus, doctor will ask about medical history, do a physical exam, and order lab tests of blood and urine samples. One blood test is the antinuclear antibody test (ANA). Most people with lupus have a positive ANA blood test.
Ankylosing Spondylitis Ankylosing Spondylitis (AS) usually starts gradually as lower back pain. The hallmark feature of AS is the involvement of the joints at the base of the spine. This is where the spine attaches to the pelvis, also known as the sacroiliac joints. Ankylosing spondylitis is more common in young men, especially from the teenage years to age 30. AS symptoms include: • Gradual pain in the lower back and buttocks • Lower back pain that worsens and works its way up the spine • Pain felt between the shoulder blades and in the neck • Pain and stiffness in the back, especially at rest and on arising • Pain and stiffness get better after activity • Pain in the middle back and then upper back and neck (after 5-10 years) With progression of AS, the spine may become stiffer. It may become difficult to bend for common everyday activities. To diagnose AS, doctor will ask about medical history and perform a physical exam. X-rays of the back looking at the sacroiliac joints may help in making an AS diagnosis. A positive blood test for HLA-B27 protein may help confirm a diagnosis.
Sjogren's Syndrome Sjogren's syndrome is an inflammatory, autoimmune disease. It can occur with other autoimmune diseases such as RA and lupus, but also on its own. Although the cause of Sjogren's is unknown, it is more common in women. Sjogren's signs and symptoms include: • Dry eyes (the glands in eyes do not give adequate tears) • Eye irritation and burning • Dry mouth (the glands in mouth do not give adequate saliva) • Dental decay, gum disease, thrush • Swelling of the parotid glands on the sides of the face • Joint pain and stiffness (rarely) • Internal organ diseases (rarely) To diagnose Sjogren's syndrome, doctor will do a physical exam and ask about medical history. Blood tests and other tests may also be performed. A simple biopsy of the inner lip or other area may help confirm the diagnosis.
Sjogren's Syndrome Venus Williams Diagnosed With Sjogren’s Syndrome
Drugs used to treat arthritis: • Painkillers (analgesics) - These reduce pain. They are used for many different types of arthritis and are often used together with other drugs. • Non-steroidal anti-inflammatory drugs (NSAIDs) - These reduce inflammation of the joint as well as pain. They are used for many different types of arthritis, often along with other drugs. • Disease-modifying anti-rheumatic drugs (DMARDs) - This group of drugs is used mainly in the treatment of rheumatoid arthritis but also in some other rheumatic diseases. They reduce pain, swelling and stiffness. • Corticosteroids (steroids) - These drugs are very effective in controlling inflammation.
NSAIDs can be very effective against inflammation, but they do not prevent tissue damage. Even when NSAIDs are controlling the inflammation, the joint or organ damage of arthritis can continue to get worse. NSAIDs only lessen pain and discomfort. They do not affect underlying disease.
Non steroidal anti-inflammatory drugs (NSAIDs) are examples of drugs that act on enzymes. NSAIDs inhibits the enzyme cyclo-oxygenase (COX) which catalyses a reaction in the biochemical pathway that results in the production of prostaglandins, important mediators in the inflammatory response.
The more an NSAID blocks COX-1, the greater is its tendency to cause ulcers and promote bleeding. One NSAID, celecoxib (Celebrex), blocks COX-2 but has little effect on COX-1, and is therefore further classified as a selective COX-2 inhibitor. Selective COX-2 inhibitors cause less bleeding and fewer ulcers than other NSAIDs.
NSAIDs can be classified based on their chemical structure or mechanism of action. Older NSAIDs were known long before their mechanism of action was elucidated and were for this reason classified by chemical structure or origin. Newer substances are more often classified by mechanism of action. Salicylates • Aspirin (acetylsalicylic acid) • Diflunisal • Salsalate
NSAIDs Propionic acid derivatives • Ibuprofen • Naproxen • Fenoprofen • Ketoprofen • Flurbiprofen • Oxaprozin Acetic acid derivatives • Indomethacin • Sulindac • Etodolac • Ketorolac • Diclofenac (Safety alert by FDA) • Nabumetone
NSAIDs Enolic acid (Oxicam) derivatives • Piroxicam • Meloxicam • Tenoxicam • Droxicam • Lornoxicam • Isoxicam Fenamic acid derivatives( Fenamates ) • Mefenamic acid • Meclofenamic acid • Flufenamic acid • Tolfenamic acid
NSAIDs Selective COX-2 inhibitors (Coxibs) • Celecoxib (FDA alert) • Rofecoxib (withdrawn from market) • Valdecoxib (withdrawn from market) • Parecoxib FDA withdrawn • Lumiracoxib TGA cancelled registration • Etoricoxib FDA withdrawn • Firocoxib used in dogs and horses Sulphonanilides • Nimesulide (systemic preparations are banned by several countries for the potential risk of hepatotoxicity) Others • Licofelone acts by inhibiting LOX (lipooxygenase) & COX and hence known as 5-LOX/COX inhibitor
NSAIDs are generally indicated for the symptomatic relief of the following conditions: • Rheumatoid arthritis • Osteoarthritis • Inflammatory arthropathies (e.g. ankylosing spondylitis, psoriatic arthritis, Reiter's syndrome) • Acute gout • Dysmenorrhoea (menstrual pain) • Metastatic bone pain • Headache and migraine • Postoperative pain • Mild-to-moderate pain due to inflammation and tissue injury • Pyrexia (fever) • Ileus • Renal colic • They are also given to neonate infants whose ductus arteriosus is not closed within 24 hours of birth • Aspirin, the only NSAID able to irreversibly inhibit COX-1, is also indicated for inhibition of platelet aggregation.
Complications of NSAIDsNSAIDs are safe drugs. However, they have many side effects. The side effects happen more often when they are used over long periods of time, which is common in arthritis patients. Some of the side effects can become very serious. • GI Effects NSAIDs irritate the gastrointestinal (GI) tract (the digestive system--your esophagus, stomach, and intestines). They increase the production of gastric acid, and they harm the gastric lining. NSAIDs aggravate ulcers and GI bleeding. Up to 5 percent of people who use NSAIDs for a year develop ulcers, bleeding, or tears in the GI tract. The risks are higher for older patients, patients with a history of GI problems, and patients with heart disease. • Blood Effects NSAIDs make it harder for the platelets in your blood to clump together at the site of an injury. This can cause bleeding problems. Aspirin especially has this effect. Before you have surgery, you should stop taking aspirin for two weeks to prevent bleeding problems. • Liver Effects NSAIDs can be toxic to your liver. You will not feel this, but elevated levels of certain liver enzymes can easily be seen in blood tests. Liver function almost always returns to normal when you stop taking NSAIDs.
Kidney Effects NSAIDs can make it hard for your kidneys to get rid of some kinds of wastes. If you have a history of kidney problems, or if your disease may affect your kidneys, your doctor will use NSAIDs with caution. • Other Effects Some people get skin reactions and rashes from NSAIDs. Some get a combination of runny nose, polyps in the nose, and asthma. Different kinds of NSAIDs can have different side effects. Salicylates can cause problems with hearing. Other kinds of NSAIDs can cause headaches and confusion, especially in elderly patients. Many of the possible side effects depend on your health and the disease for which you are being treated. Individuals can react very differently to the same NSAIDs. You and your doctor must work together to find the type and dose of NSAID that controls your symptoms without causing unwanted side effects.
CORTICOSTEROIDSCorticosteroids may regulate gene expression in several ways. Corticosteroids enter the cell to bind to GR in the cytoplasm that translocate to the nucleus. GR homodimers bind to GRE in the promoter region of steroid-sensitive genes, which may encode anti-inflammatory proteins. Less commonly, GR homodimers interact with negative GREs to suppress genes, particularly those linked to side effects of corticosteroids. Nuclear GR also interact with coactivator molecules, such as CBP, which is activated by proinflammatory transcription factors, such as NF-B, thus switching off the inflammatory genes that are activated by these transcription factors. Other abbreviations: SLPI: secretory leukoprotease inhibitor; MKP-1: mitogen-activated kinase phosphatase-1; IB-: inhibitor of NF-B; GILZ: glucocorticoid-induced leucine zipper protein; POMC: proopiomelanocortin; CRF: corticotrophin-releasing factor.
Uses of Corticosteroids • Corticosteroids are chemical copies of hormones that occur naturally in your body. The most commonly used corticosteroids are prednisone,prednisolone, and methylprednisolone. Corticosteroids can be given orally or put directly into the bloodstream through an intravenous needle. They can also be injected directly into an inflamed spot. Corticosteroid cream can be rubbed on the skin. • Corticosteroids are powerful drugs. They drastically decrease inflammation. But they are also highly toxic. Doctors have different opinions about how corticosteroids should be used. • Corticosteroids can't cure your disease. But they do seem to affect the development of some diseases, including rheumatoid arthritis (RA).
Complications of Corticosteroids Corticosteroids can have many unwanted effects on your body. Whether or not you develop these complications depends on many factors: what type of corticosteroid you take, your dose, the length of time you are on it, and how sensitive your body is to these hormones. The most common side effects are. • Osteoporosis • All corticosteroids slow bone growth and create conditions that lead to osteoporosis, a disease process that results in reduction of bone mass. Compression fractures of the vertebrae can happen with long-term corticosteroid use. Men and women past menopause are most likely to develop osteoporosis. Your doctor may recommend that you take calcium and vitamin D pills while you take corticosteroids. • Infections • High levels of corticosteroids hinder your body's ability to fight bacterial infections. High-dose corticosteroids can even mask the symptoms of some types of infections, such as abscesses and bowel tears. Most viral infections are not a problem, except for herpes. • Adrenal Insufficiency • This means that your pituitary and adrenal glands can't produce enough of certain kinds of hormones. This can happen after taking corticosteroids in moderate doses for only a few days. Adrenal insufficiency is most likely to happen as you are reducing the dosage. It can be a problem if you need surgery or if you get an infection or serious injury.
Withdrawal • When stop taking corticosteroids, the doses will be slowly reduced over a period of days or weeks. Even if patient has only been taking steroids for a few weeks, he will still need to taper off. Corticosteroid withdrawal can be very difficult for body. In many patients, the disease symptoms become worse. Some people experience a sickness that includes fevers, nausea, vomiting, low blood pressure, and low blood sugar. Others have withdrawal symptoms that include muscle and joint pain, weight loss, fever, and headaches. If patient have problems coming off corticosteroids, doctor will have taper off the drug more slowly. • Different people, and different diseases, react very differently to corticosteroids.
Contraindications to Use Corticosteroids are contraindicated in systemic fungal infectionsand in people who are hypersensitive to drug formulations. They should be used with caution in clients at risk forinfections (they may decrease resistance), clients with infections(they may mask signs and symptoms so that infectionsbecome more severe before they are recognized and treated),diabetes mellitus (they cause or increase hyperglycemia),peptic ulcer disease, inflammatory bowel disorders, hypertension,congestive heart failure, and renal insufficiency.
Disease-modifying Anti-rheumatic Drugs (DMARDs) • The early use of disease-modifying anti-rheumatic drugs (DMARDs) has been recommended in recent years to reduce disease progression and long-term disability.The need for early use of DMARDs is incorporated in new National Institute for Health and Clinical Excellence (NICE) guidance. Early use requires early referral in part because DMARD initiation is the province of specialists in secondary care. The optimum use of these drugs requires specialist experience and is complicated not only because of their potential toxicity, but also by the range and combination of drugs used. There are a number of new DMARDs.
DMARDs • The prevailing guidelines for the management of rheumatoid arthritis (RA) recommend that, once the disease has been diagnosed and its impact on the patient's life documented, DMARDs should be commenced. DMARDs should be part of a range of treatments from different professional disciplines. For further details see separate article Management of Rheumatoid Arthritis. • DMARDs either affect the immune response or suppress the disease process. As well as improving the symptoms and signs of the arthritis, they may also improve the extra-articular manifestations such as vasculitis in addition to exerting systemic effects.Any DMARD that has been prescribed should be recorded in a patient's notes, both written and electronic, so that all doctors prescribing for that patient will be aware of any potential interactions with other drugs.
Types of disease-modifying anti-rheumatic drugs DRUGS WHICH SUPPRESS THE DISEASE PROCESS Gold: • May be given either orally as auranofin or by intramuscular injection as sodium aurothiomalate. • Sodium aurothiomalate is licensed for the treatment of rheumatoid arthritis (RA) and juvenile idiopathic arthritis. • Can be an effective treatment but use is restricted by severe adverse reactions (up to 5% of recipients). • Sodium aurothiomalate has a greater toxicity than auranofin, but tends to be more effective and has a faster onset of action. • Either drug should be withdrawn if no benefit is seen after six months.
Types of disease-modifying anti-rheumatic drugs DRUGS WHICH SUPPRESS THE DISEASE PROCESS Penicillamine • It is a chelating agent licensed for the treatment of severe active rheumatoid arthritis, including juvenile forms (and a range of other conditions, including Wilson's disease). • It has a similar method of action to gold and more patients are able to tolerate it, but side-effects occur frequently. • The rate of onset of action is slow, improvement may not be seen for three months but, in patients who have shown no benefit after a year of treatment, the drug should be discontinued. Sulfasalazine • It is licensed for the treatment of RA which has failed to respond to non-steroidal anti-inflammatory drugs (NSAIDs). • It has a similar action to gold. • It has slightly more side-effects than methotrexate.
Types of disease-modifying anti-rheumatic drugs Drugs which affect the immune process Chloroquine and hydroxychloroquine • Hydroxychloroquine is an antimalarial agent licensed for the treatment of RA, juvenile idiopathic arthritis, discoid and systemic lupus erythematosus, and dermatological conditions caused, or aggravated, by sunlight. • They are usually better tolerated than gold or penicillamine. Methotrexate • May be used in the treatment of RA and psoriatic arthritis. • It is a disease-modifying agent with both anti-inflammatory and immunosuppressant activity. • It is also classified as an antimetabolite cytotoxic agent, and is the most common first-line agent for the early treatment of RA in the UK.