Download

1 / 33
330 likes | 375 Views
Explore the concept of Pay-for-Performance (P4P) in healthcare systems, focusing on incentivizing providers for improved outcomes. Learn about different designs, measures, and global experiences in implementing P4P strategies.

E N D
Pay for Performance(“P4P”) Bangkok December 2009
“Demand side” Conditional Cash Transfer (CCT) Programs ( mostly LAC) Households receive income transfers preventive care services Maternal and child care Money and food to motivate TB/HIV patients to complete treatment. “Supply side” Paying Premiums Argentina Providers “Process” Indicators = Improved Outcomes Bonus Systems Service Packages (typically primary care) Afghanistan,Haiti,Rwanda. Performance Incentivesto Households and/or Providers
“Demand side” Conditional Cash Transfer (CCT) Programs ( mostly LAC) Households receive income transfers preventive care services Maternal and child care Money and food to motivate TB/HIV patients to complete treatment. “Supply side” Paying Premiums Argentina Providers “Process” Indicators = Improved Outcomes Bonus Systems Service Packages (typically primary care) Afghanistan,Haiti,Rwanda. Performance Incentivesto Households and/or Providers
Paying Providers based on performance (P4P) • What is it? Measure performance of participating providers to set financial incentive for improving performance, leading to better outcomes Payment Incentive Performance Outcomes/Goals
Paying Providers based on performance (P4P) • What is it? Measure performance of participating providers to set financial incentive for improving performance, leading to better outcomes Payment Incentive Performance Outcomes/Goals Outputs
Paying Providers based on performance (P4P) • What is it? Measure performance of participating providers to set financial incentive for improving performance, leading to better outcomes Payment Incentive Performance Outcomes/Goals
Paying providers based on performance (P4P) • What is it? Measure performance of participating providers to set financial incentive for improving performance, leading to better outcomes Payment Incentive Performance Outcomes/Goals • Why P4P? • Improved Outcomes • In the process….reduce costs, improve quality and efficiency/equity
Pay-for-Performance (P4P)for physicians and hospitals • There are different P4P designs • Why? • Different information technology capabilities • Data availability • Willingness of providers to participate
Pay-for-Performance (P4P)for physicians and hospitals • There are different P4P designs • Why? • Different information technology capabilities • Data availability • Willingness of providers to participate • P4P is more common for outpatient care than for hospital care • Preventive and primary care services
Types of Measures: Start Here • Basic Access • Example: operating hours • Preventive Services • Number of enrollees that have a prepared annual health plan • Breast cancer screening (mammograms) • Cervical cancer screening (pap smears) • Retinal eye exams for diabetics • Well-child exams • Childhood immunizations • Institutional Capacity • Implementation of a financial management system Source: Rena Eichler, WB, 2003
Types of Measures: Extend to More System-Based • Effective management of chronic cases • Percentage of diabetics with controlled lipid levels (LDL levels less than 130mg/dL) • Health education • % of smokers who participate in smoking cessation workshops • Hospital quality • Infection rates • Control excessive utilization • Percentage of prescriptions that are generic
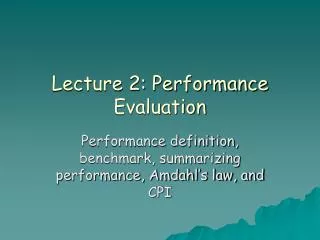
UK: Examples of Measures for Chronic Care Source: Pay for Performance Program, UK. www.nejm.org
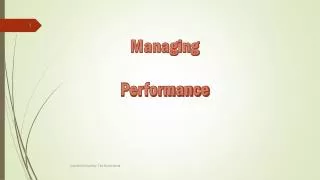
Primary Care Doctors’ Reports of Any Financial Incentives Targeted on Processes/Quality of Care, 2006 Percent reporting any financial incentive* * Receive of have potential to receive payment for: clinical care targets, high patient ratings, managing chronic disease/complex needs, preventive care, or QI activities Data: 2006 Commonwealth Fund International Health Policy Survey of Primary Care Physicians
United States • Started in private sector (80% of HMOs use) • Medicare • Bonuses to Hospitals • Top 20% for processes related to specified treatments • Joint replacement, CABG, heart attack, heart failure, pneumonia • Medicaid • 115 P4P programs in States (50 million lives) • Flat bonus or premium, withholds, publication of provider scores
United States (Maryland) • Incentives for reducing actual number of complications after hospital admissions linked to poor quality of care, such as • Urinary tract Infection • Septicemia (infection in blood) • Collapsed lung • 52 categories
Since 2004, the NHS of the UK introduced P4Pfor Family Practitioners • NHS committed $3.2 billion in additional funding over 3 years for P4P program • 146 indicators for P4P • Immunizations, well-child care • 10 chronic diseases • organization of care • patient counseling and experience • Postgraduate education allowance
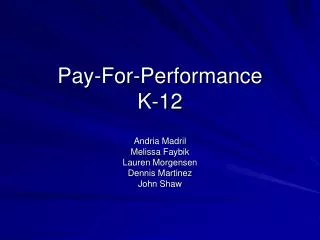
P4P: Impact on Qualityof Community Services in England Mean Scores for Clinical Quality at the Practice Level for Aspects of Care for Coronary Heart Disease, Asthma, and Type 2 Diabetes That Were Linked with Incentives and Aspects of Care That Were Not Linked with Incentives, 1998–2007. Quality scores range from 0% (no quality indicator was met for any patient) to 100% (all quality indicators were met for all patients). Source: S. Campbell et al., “Effects of Pay for Performance on the Quality of Primary Care in England,”N Engl J Med 2009;361:368-378.
Overall Results Mixed (US and UK) • Some Improvement in quality but often modest (<5%) in terms of outcomes • Not clear who benefits (US HMO PacifiCare • Top quintile of provider performance • Lowest quintile (not often) • Administrative costs higher (UK: check the box). Family practitioners (FP) employed more nurses and administrative staff and increased use of electronic medical records • Questions Remain: e.g., does it take away from non-bonus areas of care?
Results from 1st Year of P4Pin the UK • Financial incentives affect physicians’ behavior • But no way to establish how much of behavior change is due to P4P • Providers attained a median of 96.7% of available points compared to 75% predicted • Targets were too easy to achieve • P4P program increased gross income of average family practitioner by $40,200 per year • As a result, cost to payer was considerably more than expected • Smaller FP practices have merged due to administrative pressures from new P4P contract
Global budgets allocated in monthly installments • A 10% retention bonus fund for compliance with performance indicators including • Good quality (e.g., hygiene and sterilization practices) • Patient satisfaction (no overcharging and perceptions of quality) • No fraud (ghost patients) • Hire and fire staffing policies; • Staff mix flexibility/Salary adjustments/bonuses and staff/ promotions flexibility • Outcomes • Improvement in quality • general and surgical mortality • lower infection rates • Higher efficiency • improved bed turnover rates, occupancy rates, length of stay • physician hours • expenditure per admission Brazil
Haiti • Providers paid fixed fee plus bonus for achieving performance targets • Measures: • increase in % of children < 1 who are fully immunized • increase in % of pregnant women who receive at least 3 prenatal care visits • for each indicator, a baseline measure determined at the beginning of a contract period and a target for improvement is established. • Subcontracts clearly established targets, describe how performance will be measured, and determine the award fee associated with attainment of each target. • Results • 2.7 million people • Increased immunizations by 24%
An Initial List • Target physicians or facilities? • Primary or specialists? • Carrots or sticks? • Performance thresh-holds be • Absolute changes? • Relative scoring rank? • New Funding? Where will funding come from?
Different Methods to Pay Based on Performance • Withholds • Withhold about 5% of reimbursement. Return all or proportion • Bonus • Provide mean rewards ranging from 5-20% of total reimbursement • Reward top-rated providers only • Quality grants • Provide funds to provider for specific quality improvement project (e.g. access to rural residents) • Threshold • Link at least 10% of compensation to change behavior
What is Financial Riskfor providers under P4P? • Providers can gain incremental revenue from successful performance without large financial risks under P4P programs • But if P4P is budget neutral • Hospitals performing in top decile receive a 2% increment in payments, • Hospitals in second decile receive a 1% increment • Hospitals classified in lowest two deciles are liable for a 1 to 2% financial penalty
Key Messages • KISS Principle important
Key Messages • KISS Principle important • Design: • Clear performance indicators and targets need to be established • Do indicators link with outcomes? • Clear methods: the way payment will be tied to results • If not, signals for behavior change will not be clear
Key Messages • KISS Principle important • Design: • Clear performance indicators and targets need to be established • Do indicators link with outcomes? • Clear methods: the way payment will be tied to results • If not, signals for behavior change will not be clear • Administrative: • Capacity to design, negotiate, monitor and manage contracts or performance agreements
Key Messages • KISS Principle important • Design: • Clear performance indicators and targets need to be established • Do indicators link with outcomes? • Clear methods: the way payment will be tied to results • If not, signals for behavior change will not be clear • Administrative: • Capacity to design, negotiate, monitor and manage contracts or performance agreements • Stakeholders • Engagement is critical to success to assure that the design of the approach will motivate the desired results • Sufficient buy-in among recipients to generate cooperation and partnership rather than resistance.
Thank you Email: jlangenbrunner@worldbank.org Website: www.worldbank.org Health Systems Development