Download
1 / 45
450 likes | 549 Views
Explore the importance of translation in health programs, with insights on Fit and Strong! Developments, funding challenges, and future strategies for evidence-based interventions. Discover the crucial link between joint impairment and disability in older adults.

E N D
Briiiiiidging the Translation Gap and Surviving! Susan Hughes, DSW Minnesota Gerontological Society April 24, 2009
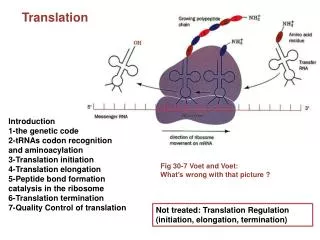
Overview • Importance of translation • Review development and testing of Fit and Strong! (EB program) • Current status translating Fit and Strong! – RE-AIM and lessons learned
Need for translation • Number of EB programs in pipeline growing • Result of substantial investment by NIH • In comparison, minimal support for translation • Major public health challenge right now • AoA and CDC stepping up to plate but $ limited
Future • Despite limits in funding, practice will have to change to incorporate EB programs that are out there • $1 billion sitting in DHHS for this purpose= down payment • Title indicates, surviving current challenges tricky but doable-
Future cont’d • fundamentally – translation/diffusion totally necessary- hope you will agree- • when times are tough, $ limited, even more important that programs offered have greatest impact possible • Now, move on, describe Fit and Strong!
First, acknowledge • Greater Chicago Chapter, Arthritis Foundation • NIAMS • National Institute on Aging Roybal Center (P50 AG15890) • National Institute on Aging (R01 AG23424) • Centers for Disease Control and Prevention (R18 DP001140) • Arthritis Foundation • Chicago Department on Aging
In what sense, evidence-based???? • Builds on earlier longitudinal study of 600 older adults in Chicago (GeriMAC) • Supported by Arthritis Foundation and NIAMS • Found: • Arthritis is number one cause of disability • Lower extremity joint impairment, in particular, is a risk factor for future disability
Converging Evidence-LE Impairment and Disability • 1990: Jette, Branch, and Berlin • LE performance predicts IADL disability at 2 years • 1995: Guralnik, et al. • LE performance at baseline predicts Year 4 ADL disability and institutionalization • 1998: Dunlop and Hughes • LE joint impairment at baseline predicts disability levels at year 4 consistent with institutional use • First to pin-point role of joint impairment due to arthritis as causal mechanism
LE Joint Impairment and Disability • Link makes sense when consider role of large, weight bearing LE joints in performing ADLs • Toileting • Transferring in/out of bed • Climbing stairs, etc.
Purpose of Longitudinal Study • Identify modifiable risk factors related to disability • Finding re LE joint impairment indicates urgent need develop intervention to interrupt progression of impairment to disability • Physical activity a likely candidate
OA Exercise Literature • People with OA have poor aerobic functioning and decreased muscle strength vs controls • Pain decreases activity; • Decreased activity leads to de-conditioning: • Frozen joints • Wasted muscles • Decreased lung and heart capacity= vicious cycle
OA lit cont’d. • Most studies targeted increased muscle strength or aerobic capacity • Recent consensus that mulitple component programs needed • Target • Flexibility/balance • Aerobic capacity • Strength
OA exercise literature, cont’d Most studies found benefits at conclusion of 8 or 12 week interventions Almost no information on longer term impact or maintenance of PA after programs ended
Adherence Literature suggests: • include education component geared to increasing self-efficacy (SE) • What is self-efficacy? • Confidence can perform a task • Belief that if you perform it, you will achieve a desired outcome • 3 types of SE important in this case: • arthritis disease management • exercise • exercise adherence
Adherence Literature suggests: • make exercise as easy to do as possible • help participants develop individualized routines • provide structured reinforcement re: progress
Combines Exercise with Education for Lifestyle Change • Can’t just tell people to exercise and teach them how • Need to review what exercise means to them in context of their lives prior experience concerns about safety facilitators and barriers problem solving
Fit and Strong! Components • Multiple-component exercise plus education for lifestyle change • 3 sessions/week for 8 weeks = 24 sessions • 60-minutes exercise, 30 minutes education
General class schedule • 5 minute warm-up • 20 minutes of aerobic exercise • 20 minutes of strength training • 10 minutes of flexibility/balance • 5 minutes of cool-down • 30 minutes-Education, group problem solving
Individualized Contract for Exercise Maintenance • Important feature: Week 7, instructor develops an individualized plan with each participant to follow after Fit and Strong! ends • Develops individualized plan incorporating preferences for time, place, form of: flexibility aerobic strength exercises Plan is a contract for post Fit and Strong! maintenance which each participant signs
Efficacy StudyDesign/Methods • RCT, will an exercise/education intervention targeted to people with lower-extremity OA: • lower extremity disability • 6-minute distance walk (aerobic capacity) • time to rise unassisted from seated position (lower-extremity muscle strength) • exercise, exercise adherence, and arthritis management SE over short term (8 weeks)?
Design/Methods (cont’d) • And, will sustained adherence to PA after Fit and Strong! ends affect outcomes at 6 and 12 months?
Pre-Posttest Measures • Baseline; 2, 6, and 12 months • called participants in both groups quarterly • still exercising? • what doing? • how long, how often?
Baseline Demographic Characteristics* • *No statistically significant differences between treatment and control groups
Other Self-Reported Conditions Treatment Control (N = 115) (N = 100) % % • Cardiovascular 36.8 33.0 Disease • Asthma 6.8 5.8 • Emphysema 3.9 5.8 • Diabetes 14.6 12.8 • Cancer 6.8 2.3
Analyses • Used Random Effects • One covariate: • Arthritis Functional Class • Found in attrition analyses to discriminate between groups
Conclusions • Benefits observed at 2, 6, and 12 months; no untoward results (rheum fellow) • Efficacy trial preliminary baseline, 2 and 6 months findings published April 2004 Gerontologist • Efficacy trial final baseline, 6 and 12 month findings published December 2006 Gerontologist
Effectiveness R01: Long-Term Maintenance of Exercise Among Older Adults with OA • Funded by NIA through cross-institute initiative to examine strategies to support long-term maintenance of behavior change • Opportunity to expand REACH of Fit and Strong!
Design and Methods • Recruit 600 older adults • Replicate Fit and Strong! in 5 Chicago Department on Aging regional senior centers with all participants • Following 8-week Fit and Strong!, participants were randomized to “mainstreamed” vs. “negotiated” treatment groups; half in each group received telephone reinforcement
Design and Methods cont’d. • Outcomes assessed in person at baseline, 2, 6, 12, and 18 months • Quarterly telephone calls assess maintenance of multiple component physical activity program over time
Changed Instructors • Prior goal: err on side of safety- designed and tested using Physical Therapist instructors • Current goal: maximize REACH/reduce cost • Trained certified exercise instructors in Fit and Strong! • 161 participants trained by PTs; 375 participants trained by CEIs.
Results of Change • Compared outcomes under two instruction modes • Hypothesis: no difference in outcomes • Found no significant differences between PT and CEI-led participants on: • Attendance • Maintenance of physical activity • Class evaluation (overwhelmingly positive for both) • Performance measures • LE Pain, stiffness, and functioning • Superior results in PT-led group on two of five SE measures: • SE for exercise and barriers adherence SE (Seymour, Hughes at al, in press, Arthritis Care andResearch)
Findings 2, 6, and 12 months: Exercise Participation (N = 486)
Conclusions • Fit and Strong! is safe, low cost, easily replicable EB program • Has been demonstrated to impact: • Exercise maintenance • Lower-extremity stiffness, pain, physical function • Lower-extremity strength (timed sit-stand) • Aerobic capacity (6 minute distance walk)
Conclusions cont’d. • Benefits observed at 2, 6, and 12 months-consistent over time • Benefits consistent across increasingly diverse participants, settings, and geographic areas
Current translation efforts • R18 from CDC to disseminate in IL and NC- working with AAAs • Contract from National Arthritis Foundation to disseminate in 4 additional states (NH, MI, KS, CA) • Active at multiple sites in WVA- mayor’s reaction! • Describe more in breakout
Bottom Line- Just Do It! • Do evidence based programming! It matters and can help your bottom line in addition to your clients over time • Researchers –hang in there- intervention-translation a long road but doable and incredibly rewarding • If we stick together- as a community of committed gerontologists, produce the evidence, send the same message -the $ will follow!