Download
1 / 24
240 likes | 548 Views
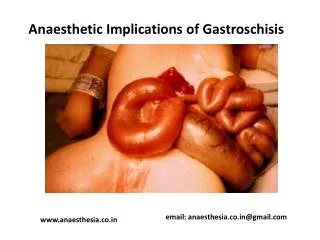
Anaesthetic Implications of Gastroschisis. email: anaesthesia.co.in@gmail.com. www.anaesthesia.co.in. Gastroschisis. An abdominal wall defect in neonates which is apparent at birth Bowel protrudes thru full thickness defect in abdominal wall adjacent to umbilical cord

E N D
Anaesthetic Implications of Gastroschisis email: anaesthesia.co.in@gmail.com www.anaesthesia.co.in
Gastroschisis • An abdominal wall defect in neonates which is apparent at birth • Bowel protrudes thru full thickness defect in abdominal wall adjacent to umbilical cord • Defect to the rt of umbilicus • No covering over bowel other than thickened, inflamed peritoneum
Gastroschisis • Hernial contents may contain entire midgut, stomach, fallopian tubes, ovaries, bladder but never liver • Asso with other cong disorders mostly of GIT like malrotation, atresia, stenosis, volvulus etc in around 16% of pts • Incidence – 1: 3000 • Requires urgent surgery as bowel is exposed making it prone to ischemia & infarction with significant fluid and heat loss.
Gastroschisis The bowel, stomach, bladder are outside abdo and completely uncovered. The umbilical cord is lateral to the small defect
Omphalocele • Also known as exomphalos. Is of two types- exomphalos major and exomphalos minor • It is presence of translucent avascular sac consisting of peritoneum and amniotic membrane, at the base of umbilical cord • Thus umbilical cord lies at the apex of the sac which may vary from few cms to huge sac containing entire midgut, stomach, liver ,spleen • Abdo cavity extremely small
Omphalocele • Muscular portion of diaphragm may also be missing • Incidence - 1:5000 • Asso with high incidence of cong defects like nonrotation, meckels d, CHD(30%), chrosomalabn, CDH, meningocele, Beckwith-Wiedemann syndrome(10%), bladd and cloacalabn • Surgery shd be performed as soon as the neonate is adequately resuscitated
Differences Gastroschisis Omphalocele Translucent avascular sac of peritoneum and amniotic memb(amnion) Umbilical cord at the apex of the sac Contents may vary from few int loops to entire midgut, stomach and liver Develops at 10 wks of i/u life d/t failure of gut to return to the abdo cavity Asso cong disorders are as high as 74% • Contents not covered by any memb: highly susceptible to infec & loss of e/c fluid • Umbilical cord lies adjacent to the sac • Liver is always inside the abdomen • Embryologically develops later in i/u life d/t tissue defect at the base of umbilical cord • Other cong birth defects rare
Diagnosis - intrauterine First trimester USG--- • With peritoneal covering– OMPHALOCELE • Without covering- GASTROSCHISIS Amniotic fluid AFP levels ---Pt with diagnosis of omphaloceleshd proceed with a early amniocentesis for chromosomal abn, and pt of gastroschisisshd have amniocentesis at 35-37 wks for lung maturity
Care at birth • Keep the exposed intestine moist & warm with saline and placing lower body in plastic bag, alternatively a single layer of povidone iodine soaked gauge is placed over the sac which is then wrapped • Prevent hypothermia- kept in heated incubator with additional O2
Care at birth • Treat hypoglycemia & acidosis • Administration of antibiotics and vit K
Preop assessment • Gestational age • Weight • Airway(difficult airway) • Respiratory status--- tachypnea, tachycardia and nasal flaring with low O2 sat due to increased work of breathing • Skin perfusion, capillary refill, HR, BP, CVP for volume status • CVS- for CHD( abn pulses, low BP, central cyanosis, murmurs, etc) • Assessment of other congenital anomalies
Preop care Major concerns- fluid loss, ventilation • Assessment of resp status & management of resp insufficiency, if present • Aggressive fluid replacement correction of deficit by 10%D in 0.2%NS + 10ml/kg/hr infusion of warmed NS or 5%albumin + boluses of 3-5ml/kg of crystalloids every 2-3 hrs to replace 3rd space losses --Adequacy checked by good peripheral circulation and urine output
Investigations • CBC • S.electrolytes • BG cross matching • ABG to assess adequacy of oxygenation and ventilation • CXR • Renal USG • Cranial USG in premature infants to rule out ICH prior to surgery
Anaesthesia • Warmed OR • Monitors/warmer to be kept ready • Gastric decompression thru NG tube • Cannulation of a vein in upper extremity and an artery, if not already present
Management of anaesthesia • No sedative premedication, atropine considered • Preoxygenation with 100% O2 • Iv / inhalational induction--- cricoid pressure--- ET tube secured • N2O avoided • Maintenance of anaesthesia with O2 + air + inhalational agents
Management of anaesthesia • Adequate oxygenation to be ensured (pao2- 80-100; spo2 97-98% in term, 87-92% in preterm • Adequate msl relaxation, atracurium preferred @0.5mg/kg • Iv opiods(fentanyl @3-5µg/kg) preferred
Intraop Intraop fluid management- • Should be isotonic-NS/RL/colloid/blood • Boluses of 10-20 ml/kg to be given to compensate for massive third space losses— HR ,BP, CVP, capillary refill ,Hb to be checked after every bolus • BT when 10% of blood loss has occured
Other intraop considerations • Primary closure– may cause ventilatory, circulatory or renal dysfunction with bowel necrosis(dec cardiac index and anuria)--- k/a abdominal compartment syndrome. Thus peripheral circulation shd be observed carefully & surgeon shd be alerted in time • Alternatively bowel left extraperitonealy encased in skin / silicon mesh and corrected in a second stage surgery ------- each case to be individualised depending on size of abdo cavity, and amount of herniated contents
Post op management Depends on- • Magnitude of defect • Type of repair • Associated pathology Extubation immediately after surgery may be attempted in pts with adequate respiration & hemodynamics with vigorous movements of limbs having -small primary closure -silicon mesh t/t
Post op • However in pts with large defects, along with compromised circulation, mechanical vent with msl relaxation is continued until abd pressure decreases to cause no respiratory / circulatory compromise(may take up to 3-7 days) • Weaning attempted only after decompression of abdo when baby is able to have sustained spontaneous respiration & oxygenation
Post op • Post op TPN is required for long time as bowel is edematous due to manipulation & is slow to resume its function (it takes 2 wks to 3 months for the neonate to start accepting oral feeds) • Watchful for complications like NEC, renal insufficiency, abdominal wall cellulitis & breakdown, pueumonia, etc • Hypotension, hypothermia, analgesia managed accordingly
References • Pediatric anesthesia- George A. Gregory (4thed) • Miller’s anaesthesia- 6th edition • Wylie and Churcill- A practice of anaesthesia, 7th edition • Barash • Yao & Atrusio anesthesiology • Swenson’s pediatric surgery- 5th edition • IJA- October 2004
thank you www.anaesthesia.co.in