Download
1 / 30
370 likes | 1.25k Views
Universidade Nova de Lisboa Escola Nacional de Saúde Pública. Gender inequality in health care. Ana Fernandes Julian Perelman Céu Mateus Meeting of the Aachen Group Sintra, 9-10th April 2006. Common Values. General focus. Health services achieving Universality Solidarity

E N D
Universidade Nova de Lisboa Escola Nacional de Saúde Pública Gender inequality in health care Ana Fernandes Julian Perelman Céu Mateus Meeting of the Aachen Group Sintra, 9-10th April 2006
Common Values General focus • Health services achieving • Universality • Solidarity • Equity in access/outcomes • Health policies • Promoting adequacy of health services • Sensitive to the changing health needs of citizens
Dimensions of inequality Socio-economic: - income - education - profession V e c t o r s o f a n a l i s y s Mortality Health Morbidity Use Health care provision Geographic: - regions - counties - municipalities Access Resources’ source Funding • Age • Gender Resources’ allocation
Research on gender inequalities in health care Inequalities in access / treatment for: • Cardiovascular diseases • Cerebro-vascular diseases (stroke) • Diabetes • Dialysis and kidney transplant • Screening for lung cancer • HIV/AIDS (access to antiretroviral therapy) • Higher use of pharmaceuticals among women
Cardiovascular diseases: Gender inequalities in treatment • In early stage (before AMI) women have lower access to: • non-invasive procedures (stress test) • diagnostic high-technology procedures (angiography) • revascularization (PCI or bypass) • In admissions for acute myocardial infarction: • lower access to bypass, but equal or higher access to PCI • higher mortality and harder recovery for women after bypass • several studies do not ascertain any gender inequality in access to high-tech treatment
Cardiovascular disease: causes for gender inequalities in treatment • Lower access related to women’s lower socio-economic status (lower access to private insurance, out-of-pocket payments, poorer information) • Physician’s discrimination • Subjective • Objective – due to higher difficulty in interpreting or targeting symptoms (male-oriented research and guidelines) • Higher reluctance by women to follow invasive treatments
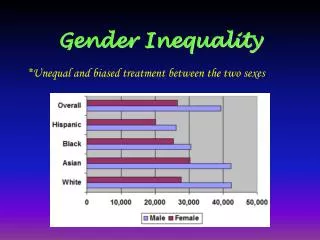
Socio-economic inequality related to gender • In all OECD countries, women have, on average, a lower socio-economic status than men • In 2002, in Portugal, the average monthly income was € 601 for women and € 747 for men
Women's average pay as % of men's - 2004 Notes: figures are for 2004 except * 2002, ** 2000, *** 2003, **** 1998, ***** 2001 ; Source: EIRO
Pro rich Pro poor Inequity in access to general practitioner
Pro rich Inequity in access to general specialist
Women’s health Main priorities when studying women’s health • Main causes of death • Diseases with a higher prevalence • Reproductive health • Violence against women • Health determinants Chesney and Ozer, 1995
Women’s health Main priorities when studying women’s health • Main causes of death • Diseases with a higher prevalence • Reproductive health • Violence against women • Health determinants Chesney and Ozer, 1995
Main causes of death • Cardiovascular diseases • Stroke • Female cancers (breast, uterus & cervix, ovary) • Cancer of colon and rectum • Lung cancer Sources: http://www.euro.who.int/ P. Boyle* & J. Ferlay Annals of Oncology 16: 481–488, 2005
Age-standardized death rates from cardio-vascular disease, women aged 35-74, latest available year Source:World Health Organization (2004) http://www3.who.int/whosis/menu.cfm www.heartstats.org
Age-standardized death rates from stroke, women aged 35-74, latest available year Source:World Health Organization (2004) http://www3.who.int/whosis/menu.cfm www.heartstats.org
Source: Atlas of Health in Europe, 2003 http://www.euro.who.int
Source: Atlas of Health in Europe, 2003 http://www.euro.who.int
Source: The European Health Report, 2005 http://www.euro.who.int/ehr2005
Women’s health Main priorities when studying women’s health • Main causes of death • Diseases with a higher prevalence • Reproductive health • Violence against women • Health determinants Chesney and Ozer, 1995
Diseases with higher prevalence • Chronic diseases and mental health diseases Chronic diseases in Portugal Source: National Health Survey, 1998/99, ONSA
Women’s health Main priorities when studying women’s health • Main causes of death • Diseases with a higher prevalence • Reproductive health • Violence against women • Health determinants Chesney and Ozer, 1995
Source: Atlas of Health in Europe, 2003 http://www.euro.who.int Source: Atlas of Health in Europe http://www.euro.who.it
Source: Atlas of Health in Europe, 2003 http://www.euro.who.int
Source: Atlas of Health in Europe, 2003 http://www.euro.who.int
Women’s health Main priorities when studying women’s health • Main causes of death • Diseases with a higher prevalence • Reproductive health • Violence against women • Health determinants (tobacco and alcohol consumption, physical activity, etc.) Chesney and Ozer, 1995
Women’s health Women’s health is an issue that goes well beyond gender inequalities in access and treatment
European Health Report 2005 “Differences across countries and population groups indicate how much impact policies to prevent and control major risk factors could have”
Research Outline for Portugal • Inpatient administrative data • Waiting lists • IMS • Outpatient administrative data (GP, specialists care)
Discussion • To reduce gender inequality in health care, socio-economic inequalities have to be addressed • To tackle gender-related inequalities, health policies will vary according to relevant inequalities • a strong effort should be put on ascertaining causes and relevance of differences • Research on gender inequalities in health care related to access and to treatment is not conclusive • Systematic comparison of women’s health conditions and assessment of health policies promoting gender equality should figure in the agenda of a European Institute for Gender Equality.