Low Tidal Volume Ventilation Data Collection
Low Tidal Volume Ventilation Data Collection. Hisham Humsy , RRT Brad Winters, Ph.D. M.D. What is Low Tidal Volume Ventilation (LTVV)?. Simply: Targeting a Tidal volume of 4-6 ml/kg of predicted body weight Not ideal body weight Not actual body weight Predicted body weight based on height

Low Tidal Volume Ventilation Data Collection
E N D
Presentation Transcript
Low Tidal Volume VentilationData Collection HishamHumsy, RRT Brad Winters, Ph.D. M.D.
What is Low Tidal Volume Ventilation (LTVV)? • Simply: • Targeting a Tidal volume of 4-6 ml/kg of predicted body weight • Not ideal body weight • Not actual body weight • Predicted body weight based on height • Avoiding the use of Zero Positive end-expiratory Pressure (ZEEP) • Use PEEP settings ≥ 5 cmH20 Armstrong Institute for Patient Safety and Quality
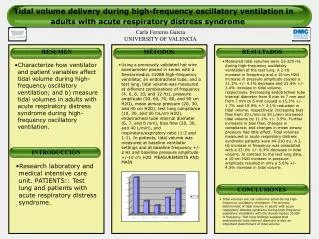
Why should we use it? • Lung Protection • “Volutrauma” • Barotrauma • Ameliorate activation of chemical inflammatory mediators • Prevent development of ARDS • Improve oxygenation • Improve outcomes • “ARDSNET” Trial compared outcomes using traditional tidal volumes (>10 cc/kg) to lower volumes (4-6cc/kg) finding significant benefit. • Several more studies and a meta-analysis led to the conclusion that large Vt and the high pressures it generates were harmful. Armstrong Institute for Patient Safety and Quality
How is it different from what is often used? • Traditional ventilation strategies use large Vt • 10-12 ml/kg • However, this approach has been shown to increase morbidity and mortality in critically ill patients, esp. those with ARDS • Large Vt results in over-distension of some areas • This leads to inflammatory responses that damage the lung Armstrong Institute for Patient Safety and Quality
Why the PEEP? • Use of Positive end-expiratory pressures (PEEP) of ≥ 5 cm H20 is recommended along with the low Vt • PEEP helps to prevent alveolar collapse at these low Vt, preventing atelectasis and “volutrauma” • How much PEEP? • Exact setting needed is unclear • It is clear is that zero PEEP (“ZEEP”) is to be avoided. • ≥5 cm H2O is the goal Armstrong Institute for Patient Safety and Quality
Who should get LTVV? • Anybody who meets criteria for Acute Respiratory Distress Syndrome (ARDS) or Acute Lung Injury (ALI) should receive this therapy. • The clinical evidence is quickly mounting that most if not all patients on mechanical ventilation, whether in the ICU or the operating room, would benefit from a LTVV strategy. Armstrong Institute for Patient Safety and Quality
Benefits • This is why applying this strategy is crucial • Tracking adherence to this strategy is an important element in improving patient safety and quality for mechanically ventilated patients. • Potential benefits: • Less lung injury • Less time on the ventilator • Reduce ICU/Hospital LOS • Reduced costs • Reduced VAE Armstrong Institute for Patient Safety and Quality
Stakeholders in LTVV • Physicians • Nurses • Respiratory Therapy Armstrong Institute for Patient Safety and Quality
Poll 1 • Is an RT a member of your CUSP team? • Yes • No • I don’t know • Not on the CUSP team, but RTs are actively involved in the clinical side of the project Armstrong Institute for Patient Safety and Quality
Poll 2 • If an RT is not a member of your CUSP team, do you think the RTs can be engaged to participate? • Yes • No • I don’t know • RT is already participating • We don’t have RTs in our facility Armstrong Institute for Patient Safety and Quality
Poll 3 • Has your team focused on LTVV in the past? • Yes • No • We are already focusing on LTVV • I don’t know Armstrong Institute for Patient Safety and Quality
Poll 4 • If not, do you think your unit would be interested in implementing LTVV as an area of improvement? • Yes • No • I don’t know Armstrong Institute for Patient Safety and Quality
Respiratory Therapists • RT has their “hands on the till” • Set up the vents • Program the settings • Alert nurses/physicians to ineffective ventilation • Offer guidance on options for adjusting parameters or trying other modes/strategies • Track and document all of the vent parameters; Vt, PEEP, PIP, Plateau Pressures, cuff pressures, secretions etc. etc. etc. Armstrong Institute for Patient Safety and Quality
Respiratory Therapy • The information necessary to ensure all patients who deserve LTVV get it (closing the “quality gap”) is right in the hands of Respiratory Therapy • You are the ventilator experts • RT’s can and should be the drivers for closing this quality gap Armstrong Institute for Patient Safety and Quality
Translation into Practice • Closing the Quality Gap • It is estimated that less then half of ARDS patient get low Vt applied in their care • A much smaller fraction of “at-risk” patients likely receive this therapy • If all patients on a vent deserve this strategy then we have a long way to go • Focusing on adaptive change, that is how we do our work, is essential to closing this gap Armstrong Institute for Patient Safety and Quality
What should Respiratory Therapists do? • Technical and Adaptive work • Technical work is what we do • The choice of tidal volume, PEEP, etc. • Adaptive work is how we do it • Ensuring that the technical work gets done appropriately • That everyone has a role in the process of communication that gets the technical work done Armstrong Institute for Patient Safety and Quality
Start by knowing your baseline • Get a baseline on how your units are doing applying LTVV strategy • Need to know where you started to know if you have improved • Use the LTVV Data Collection tool to get this baseline and track the effectiveness of your interventions. Armstrong Institute for Patient Safety and Quality
LTVV Data Collection Tool Armstrong Institute for Patient Safety and Quality
Close up Armstrong Institute for Patient Safety and Quality
Data Entry Armstrong Institute for Patient Safety and Quality
Ventilator Mode • Group 1: Volume cycled modes • Continuous Mandatory Ventilation (CMV) • Assist Control (AC) • Synchronized intermittent mandatory ventilation (SIMV) • Volume Support (VS) • Pressure Regulated Volume Controlled (PRVC) • Group 2: Pressure cycle modes • Pressure Support (PS) • Continuous Positive Airway Pressure (CPAP) • Pressure control (PC) • Airway Pressure Release Ventilation (APRV) • Bilevel ventilation • Group 3: • Proportional Assist Ventilation (PAV) • Adaptive support ventilation (ASV) • Inverse Ratio Ventilation • High Frequency Oscillatory Ventilation (HFOV) • Extracorporeal Membrane Oxygenation (ECMO) • Other Armstrong Institute for Patient Safety and Quality
Tidal Volume • Tidal Volume:Enter the Tidal Volume in milliliters (mL). • Ventilator modes are on the back of the tool • Group 1 - Use the Preset tidal (prescribed) volume if the mode is in Group 1 • Group 2 - Please enter the approximate expired tidal volume. • Group 3 - you should not be collecting this data. Armstrong Institute for Patient Safety and Quality
Plateau Pressure • Plateau Pressure: • Enter the Plateau Pressure at or nearest to the time of observation. • If unavailable or unknown please enter NA. • For APRV/Bilevel modes this is the Phighvalue. • If Group 3, you should not be collecting this data. Armstrong Institute for Patient Safety and Quality
PEEP (Positive End-Expiratory Pressure) • PEEP: • Enter PEEP value at time of observation. • If there is no PEEP value, enter “0”. • For APRV/Bilevel modes this is the Plow value. • If Group 3, you should not be collecting this data. Armstrong Institute for Patient Safety and Quality
Does the Patient have a Risk Factor for ARDS? • If the patient has one or more of the following conditions enter “Y”, otherwise enter “No”. • Pneumonia • Sepsis, Severe Sepsis or Septic Shock not secondary to pneumonia • Aspiration • Trauma Armstrong Institute for Patient Safety and Quality
ARDS? • Does the Patient have the diagnosis of ARDS at the time of the observation? • Enter Yes or No • If not easily available, ask physician and/or nursing staff • Excellent segue to Adaptive Work Armstrong Institute for Patient Safety and Quality
CUSP • Become an active member of your CUSP Team • Ventilator safety and quality is an area that is often overlooked • It is the role of the RT to make sure it is addressed by the CUSP Team • Fill out the Staff Safety Assessment with your concerns • Help your CUSP Team with: • accidental extubation issues • SAT • SBT • LTVV • Sedation issues affecting weaning • Early mobilization Armstrong Institute for Patient Safety and Quality
Adaptive Work • Once you have baseline data (will discuss reports shortly) • Work with other stakeholders to develop an intervention to improve • process for evaluating every patient for LTVV strategy • Daily Goals • Automatic order sets • Respiratory Therapy screening and clearance of vent orders to be sure they comply with LTVV • Other locally developed strategies Armstrong Institute for Patient Safety and Quality
Adaptive Work • Respiratory Therapists • Work with nursing to create easy access to height measurements for Vt calculations at time of initial vent settings • Work with doctors to make diagnosis or risk for ARDS public knowledge • Again part of daily goals? Other? • Create process to inform doctors if plateau pressures are high or PEEP was not ordered etc. • Empower RTs to make changes to meet LTVV strategy if physician is not available pending physician review Armstrong Institute for Patient Safety and Quality
Data • Data collected for LTVV should be uploaded into the CECity online platform • Enter height in either inches or centimeters • Conversion takes place automatically for calculations • Reports generated: • Compliance rate for LTVV • Compliance rate for avoiding ZEEP (PEEP >5) • Distribution of tidal volume and PEEP values • Subset compliance rates for patients identified as having ARDS Armstrong Institute for Patient Safety and Quality
Feedback • Download reports regularly from CECity • Create process to share data with the unit, CUSP team senior exec, doctors, nurses, other RTs. • Make it public! Post it! Report it! Discuss it! • Make iterative improvements to optimize your compliance • Analyze your process for barriers if you aren’t achieving your goals • Work with your IT folks to track if your vent days, LOS etc. are reduced as you close the quality gap. Armstrong Institute for Patient Safety and Quality
Questions?Comments? • Let us know your • Concerns • Ideas • Anticipated barriers • Possible implementation techniques Armstrong Institute for Patient Safety and Quality